
Surveying Oklahoma’s behavioral health workforce
Nearly 14,000 behavioral health care professionals are licensed in Oklahoma. These nurses, social workers, therapists, psychologists, physicians, and other professionals deliver critical services in the treatment of, and recovery from, mental illness and substance use disorders. Whether in independent private practice or as part of a larger hospital system, nonprofit organization, or publicly funded treatment setting, providers are the foundation of Oklahoma’s behavioral health care system.
However, many Oklahomans face significant barriers to receiving behavioral health care. The geographic distribution of providers, type of health insurance, and limited numbers of specialists affect the accessibility of Oklahoma’s behavioral health workforce.
To better understand this accessibility, Healthy Minds Policy Initiative conducted a survey of Oklahoma’s licensed behavioral health care providers. The survey received 622 responses from providers across the state.
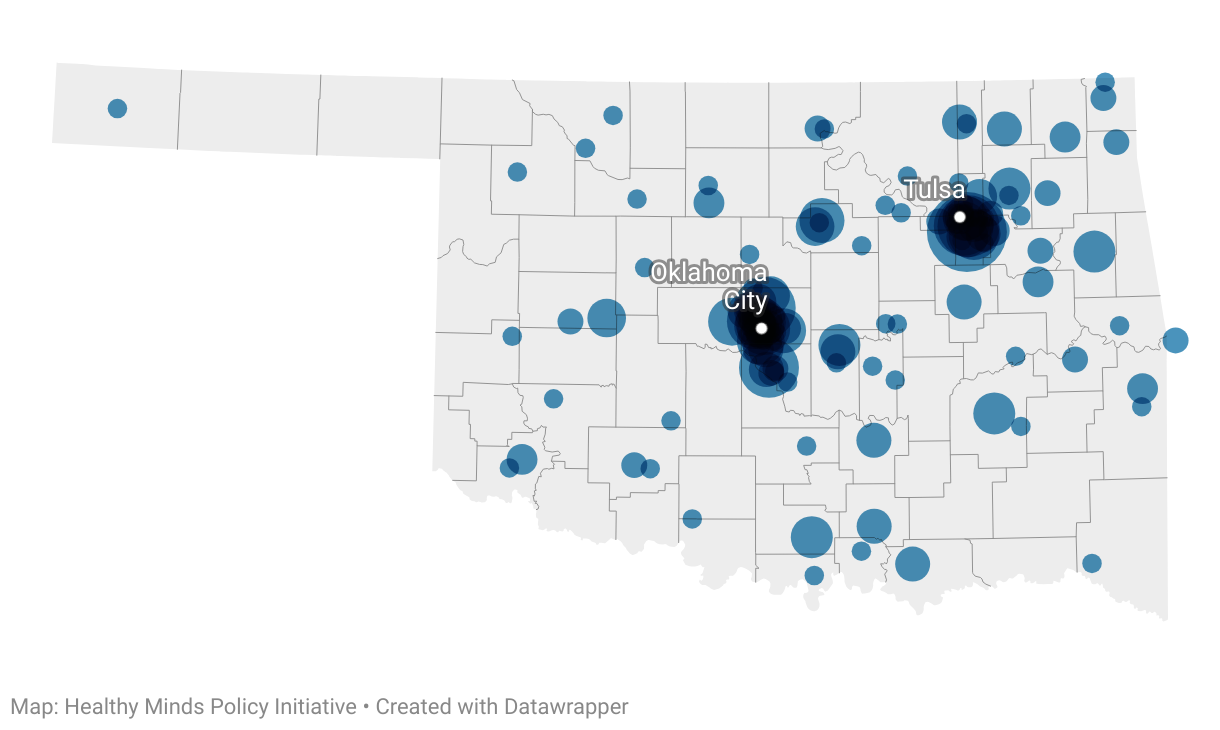
Actively Practicing Survey Respondents by ZIP Code
The survey finds that:
- A patient's inability to pay out of their own pocket significantly limits provider choices. Relatively few private practice providers who took the survey accept public insurance like Medicaid, and most favor self-pay over private insurance.
- Oklahoma's provider workforce may appear more robust than it is – 26% of surveyed providers report seeing patients only on a part-time basis.
- Patients who can afford to see a provider often have to wait. Nearly 40% of providers said they were scheduling out longer than one week, and 10.5% said they were scheduling out longer than a month. Providers who can diagnose conditions – psychiatrists and psychologists – had the longest wait times.
- Insufficient compensation for behavioral health care professionals in Oklahoma discourages new providers from practicing in the state and hurts the retention of current providers.
Background: Oklahoma's Behavioral Health Workforce
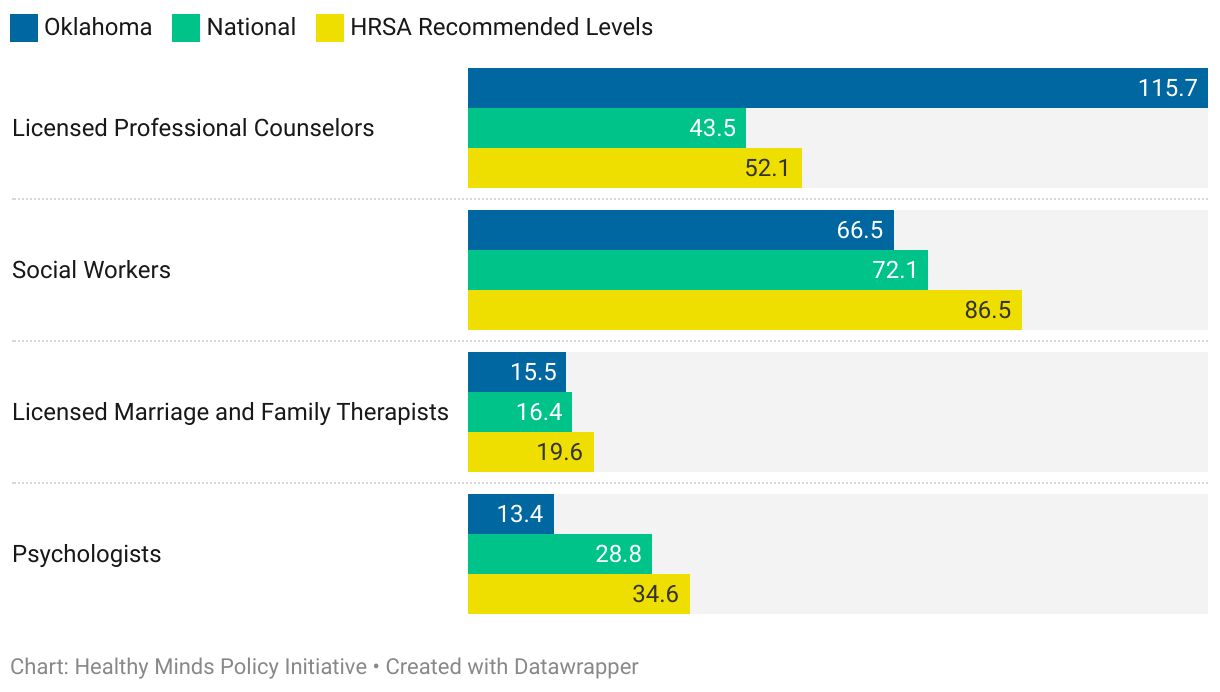
In previously published research on the availability of Oklahoma's behavioral health workforce, Healthy Minds identified only two types of providers available in the state at a per-capita rate above the national average: licensed professional counselors (LPCs) and alcohol and drug counselors. There are shortages of every other kind of licensed behavioral health care provider compared to levels recommended by the federal Health Resources and Services Administration. Rural areas of the state are in particular need of more people in the mental health workforce.
Behavioral Health Care Providers Per 100,000 People
Even if Oklahoma did have adequate availability of providers to meet its residents’ mental health needs, many other factors affect whether care is truly accessible. Health care consumers must first determine the type of services they need and which type of provider can best meet those needs. Each provider type has a specific set of skills and scope of practice, ranging from assessments and evaluations to therapy and medication management.
Although some consumers utilize a primary care provider or case manager in their search, others rely on the internet or referrals from friends and family. Insurance companies produce provider directories that are meant to help consumers find care, but these directories often have incorrect or missing information. Travel time and distance is another significant barrier, particularly for rural Oklahomans. Telehealth provides an alternative when traveling to the closest provider may not be feasible, though this requires the patient to have a reliable internet connection. Furthermore, providers might not accept new patients, only see patients within a specific age range, exclusively see patients with treatment needs that align with their specialty, or only accept certain types of insurance. These barriers are even higher for people with culturally and linguistically diverse needs.
Survey Findings
Insurance Coverage Has a Significant Impact on Consumers' Choices
Roughly 44% of practicing survey respondents said they were in independent private practice compared to practicing in a community, inpatient, or nonprofit setting. For the purpose of this survey, community, inpatient, and nonprofit settings include Certified Community Behavioral Health Centers, correctional facilities, hospitals, inpatient psychiatric hospitals, inpatient substance use treatment centers, nonprofit organizations, primary care settings with integrated behavioral health services, K-12 schools, state hospitals, university or college counseling centers, Veterans Administration facilities, and Indian Health Services facilities.
Independent private practice providers are 2.3 times more likely not to accept new patients compared to all other types of providers and twice as likely to be considered in-network on commercial insurance plans than public plans. In other words, if someone with public insurance (e.g., Medicaid) tries to see a private independent practice provider, they are more likely to incur out-of-pocket costs than someone with commercial insurance.
Payer Sources Accepted by Actively Practicing Survey Respondents
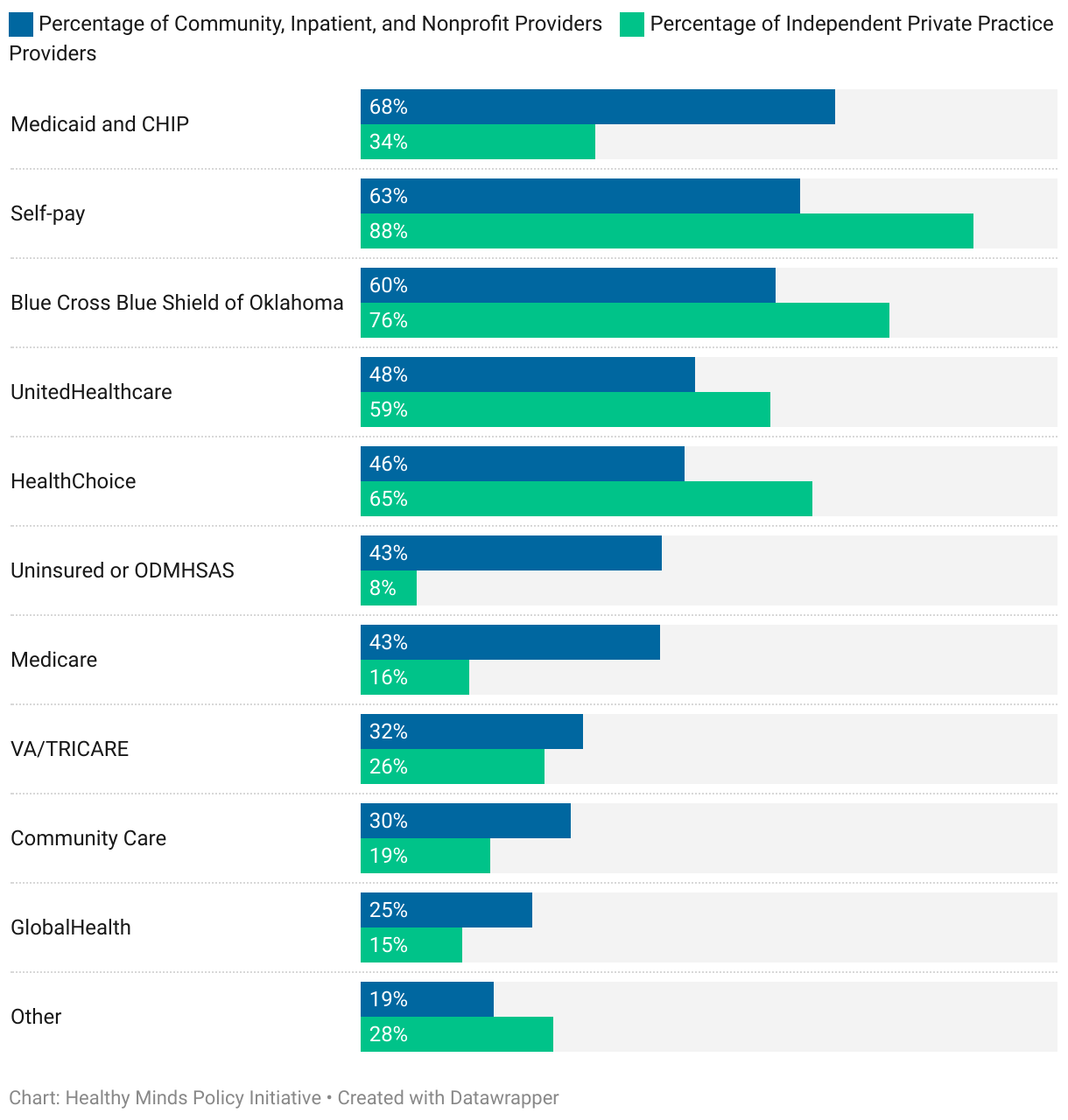
Of all payer sources, self-pay is the most commonly accepted by independent private practice providers. These providers are 1.4 times more likely than community, inpatient, and nonprofit providers to bill and receive compensation from the patient directly. Medicaid and the Children’s Health Insurance Program (CHIP) – operated as a combined program in Oklahoma known as SoonerCare – is the most common form of payment accepted by community, inpatient, and nonprofit practice providers. Among survey respondents of this provider type, 68% accept Medicaid and CHIP compared to only 34% of independent private practice providers who do.
SoonerCare covers some of the most vulnerable people in the state, including the aged, blind, and disabled, as well as children and pregnant women who fall below certain income thresholds. Those who qualify for Medicaid or CHIP are more likely to have co-occurring physical and mental health conditions and experience non-medical factors that impact health outcomes. Having access to fewer providers as a result of insurance coverage type disproportionately affects those who might already have more complex needs.
Many Providers Do Not See Patients Full-Time
A quarter of surveyed providers report spending 20 hours or less per week providing behavioral health services to clients. This indicates that many Oklahoma providers may only practice part-time, which should be considered when determining the adequacy of insurance networks. Providers may also limit their time with patients to complete administrative tasks, collaborate with peers, and/or consult on mental health cases managed by primary care practitioners. As physicians continue implementing collaborative and integrated care models, appropriately compensating behavioral health professionals for their roles on care teams will help extend Oklahoma's existing health care workforce.
Appointment Wait Times Are Longest for Psychiatrists and Psychologists
Of actively practicing survey respondents, 37% said it takes a week or more for a patient to get an appointment, and nearly 4% are not currently accepting new patients. In particular, 23% of psychiatrists reported it takes one to three months to get an appointment, and 27% of psychologists said that it can take one to six months or longer for a patient to secure an initial appointment.
Patient Wait Times for Appointments by Provider License Type
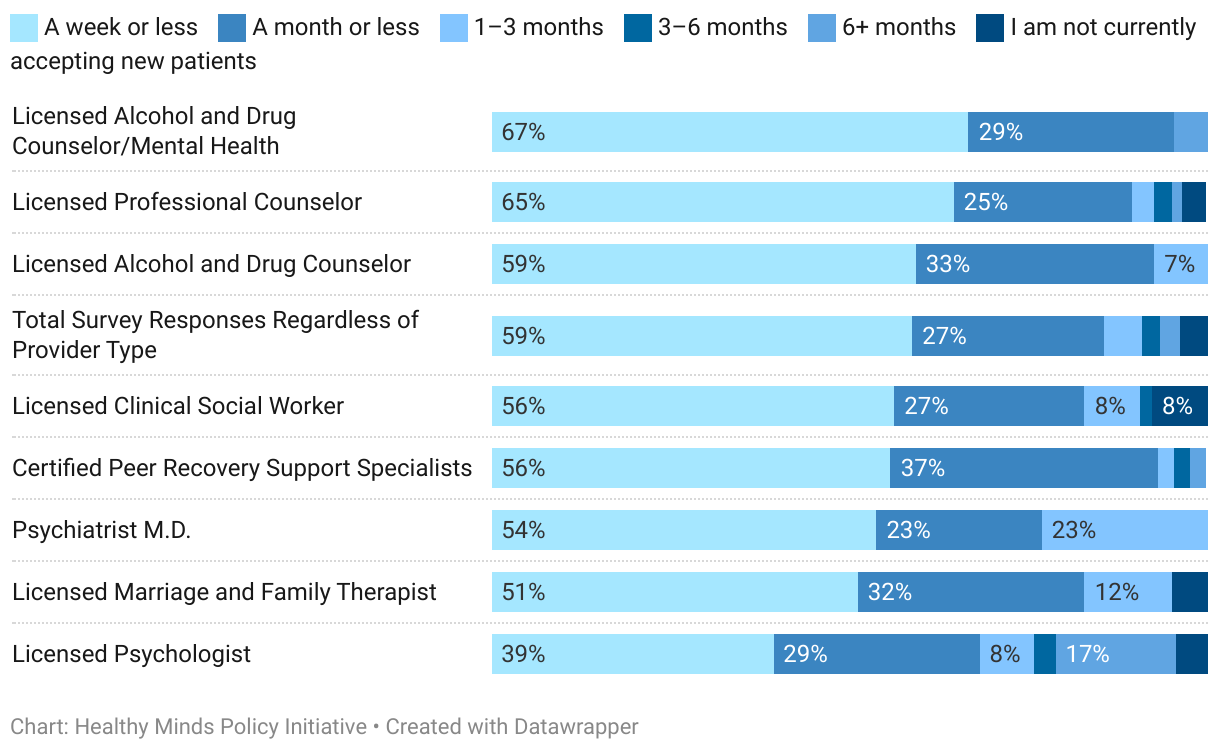
Psychologists and psychiatrists commonly diagnose mental health conditions and provide a set of services other licensed professionals cannot. Psychologists administer particular tests and assessments to arrive at a diagnosis or direct treatment. Psychiatrists, as prescribers, often see the same patients on rotation for medication management, which can leave little margin for them to see new patients.
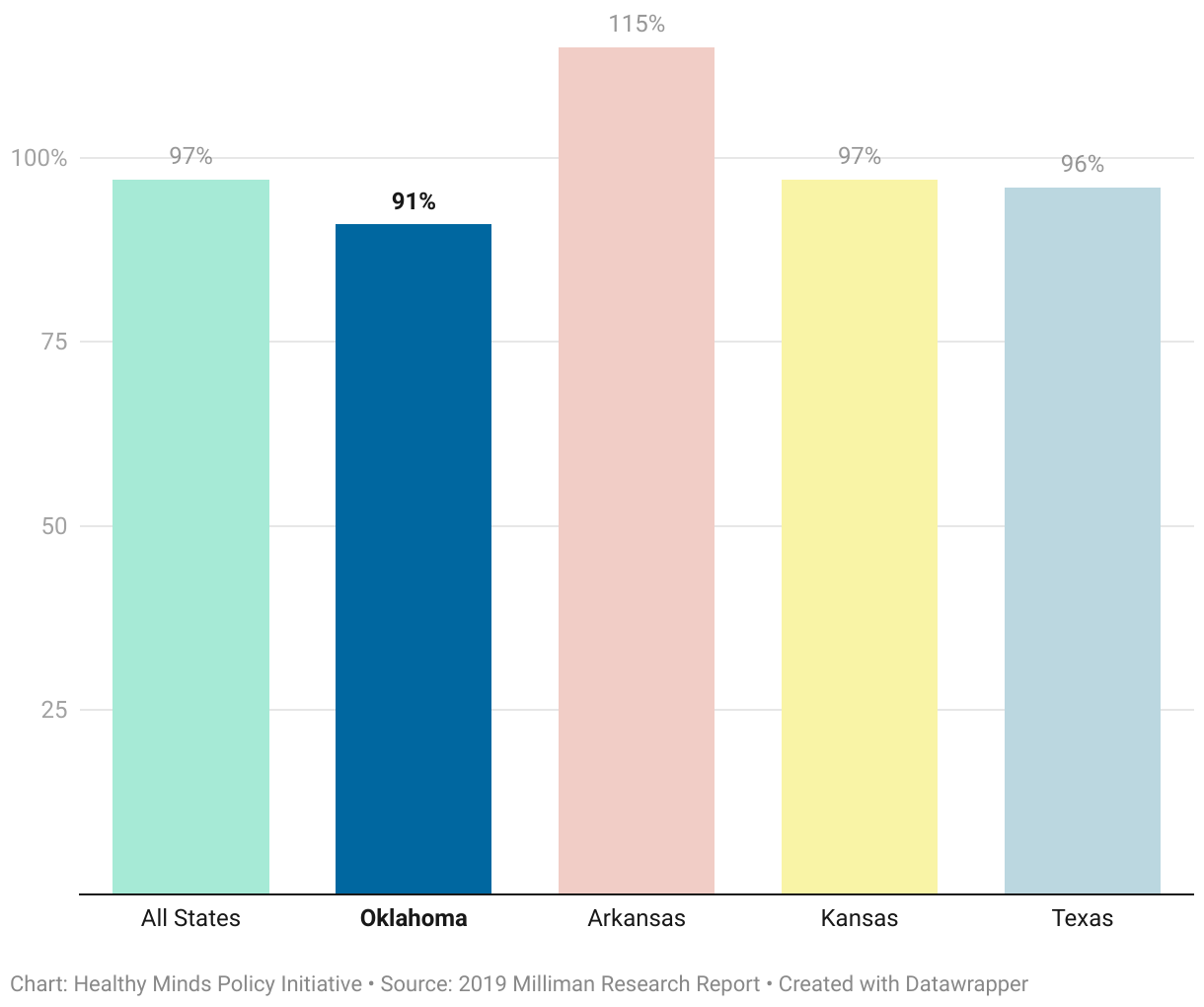
Compensation for Behavioral Health Care Lags Behind Neighboring States
A national report from 2019 shows Oklahoma's in-network behavioral health reimbursement levels relative to those allowed by Medicare are below the national average and below the levels of Arkansas, Kansas, and Texas. Medicare reimbursement levels are a benchmark in the health care industry for ideal reimbursement levels. Oklahoma behavioral health care providers that are in-network on commercial PPO plans are reimbursed on average 9% less than what is allowed by Medicare for office visits.
Average Reimbursement Rates for In-Network Behavioral Health Care Relative to Medicare-Allowed Levels
The disparity in reimbursement rates between Oklahoma's primary care and behavioral health care providers is 1.1 times higher than the national average. The state's behavioral health care providers are reimbursed an average of 27% less than primary care providers for similar visits. Oklahoma’s disparity is 13.5 times higher than that of Arkansas, where primary care providers receive only 2% more than behavioral health providers for similar services.
Former mental health care providers who responded to Healthy Minds' survey report insufficient pay as the No. 1 reason that best describes why they left the workforce. However, only 4.3% of survey respondents indicated they were either “not in behavioral health care, but still in the social services sector” or “not in behavioral health care, and not in the social services sector.” This equates to an extremely small sample of licensed providers in the state who are not currently providing direct services and should not be taken as representative.
Nonetheless, Oklahoma has room for improvement to catch up with the national average and its regional neighbors. Raising reimbursement rates for behavioral health providers would likely make Oklahoma more appealing and competitive for practitioners.
Methodology
The 21-question survey included the following topics: license type, whether or respondent provides direct services to clients, geographic areas of practice, utilization of telehealth, treatment setting, number of hours spent per week providing direct services, patient ages served, treatment specialty, typical length of time to see a new patient, accepted payer sources, and which for which insurance companies respondent is in-network.
Once the survey was created, licensure boards and provider associations either sent information about the survey to providers or shared contact information for Healthy Minds to contact individuals directly via email. Participation was optional, and providing identifiable information was optional. Even if licensure boards were unable to provide contact information for providers, all licensure boards for each type of license included in the survey were able to provide a list of actively licensed providers with either an associated zip code or county.
Of Oklahoma's 13,859 licensed behavioral health care providers, a total of 622 actively licensed providers responded for a survey response rate of 4.5%.
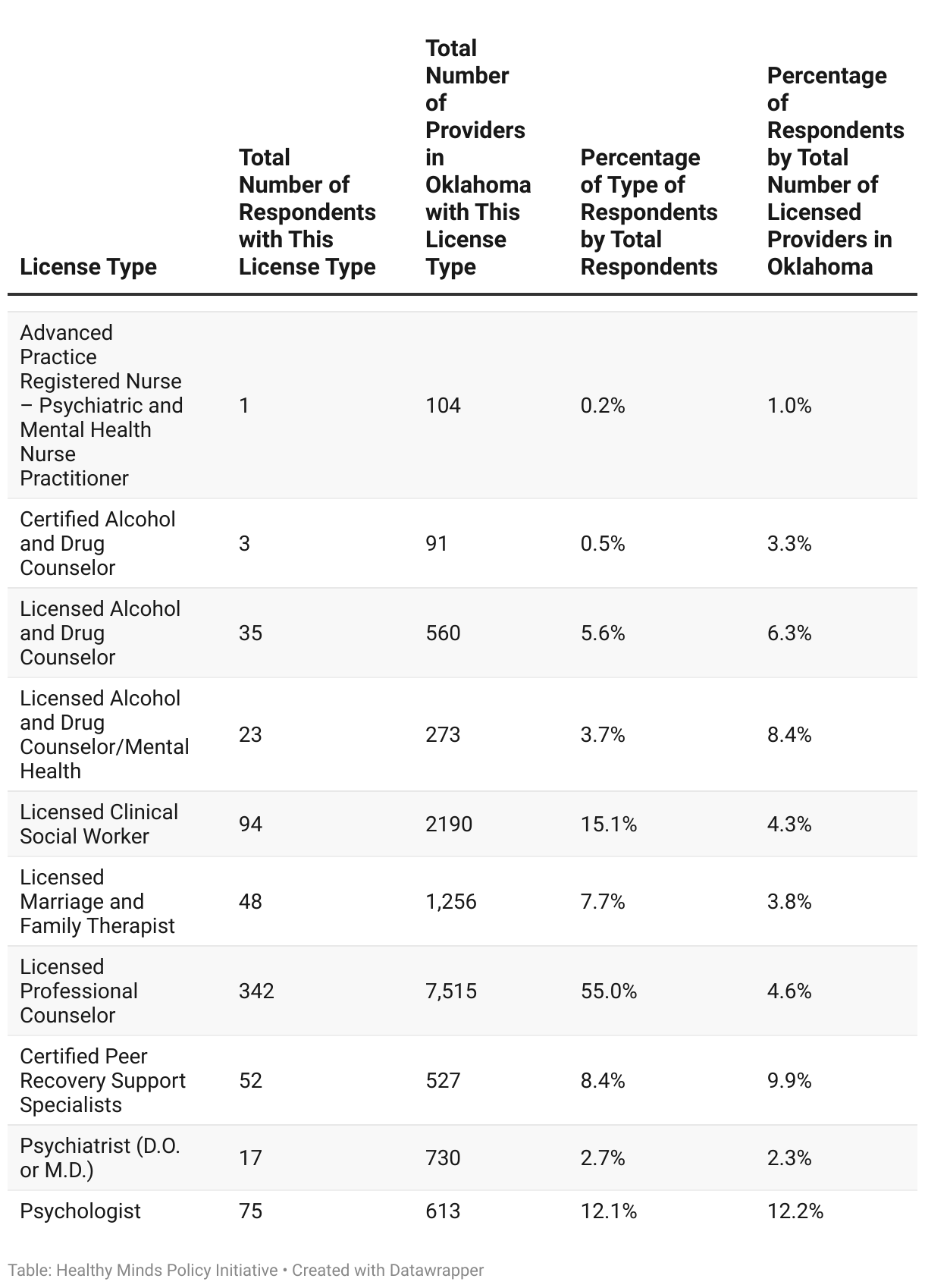
For psychiatrists, the total number of providers in Oklahoma and related survey respondent rate cover both D.O.s and M.D.s with psychiatric specialties, which include child and adult psychiatry and addiction medicine.
Respondents were allowed to select all license types that applied. Slightly more than 10% of respondents had at least two licenses or certifications, and 0.6% of respondents held at least three licenses or certifications. When an individual held more than one license or certification, that provider’s responses were counted for each unique license type in the analysis by license type, but only once per respondent for analysis for total survey responses regardless of license type. While this is not a randomized or representative sample, this duplication likely overestimates the access to service, as someone with multiple credentials is only a singular provider.
