Investing in Oklahoma's future by preventing behavioral health problems
How Oklahoma can achieve a healthier state through proven strategies to prevent mental illness and substance use
Most mental health conditions develop early in a person’s life — about half begin by age 14. But many of these problems are preventable: early, upstream “primary” prevention programs are proven to stop problems like anxiety, depression, and substance use, from ever occurring.
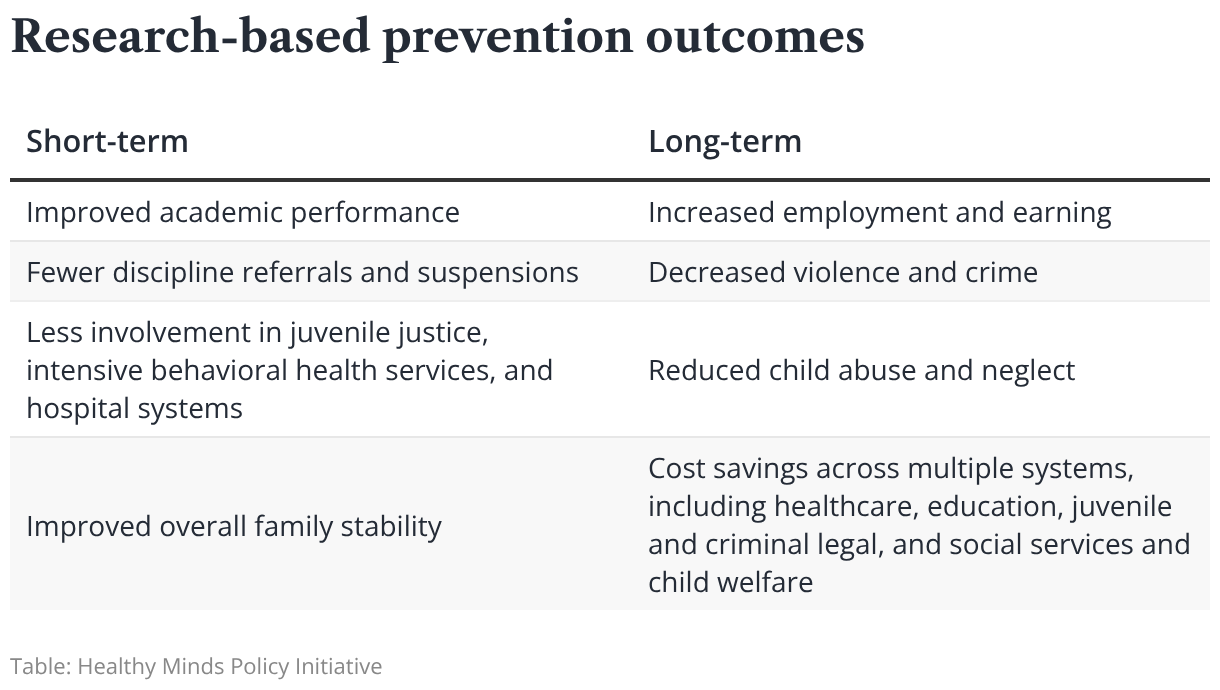
When fewer people develop behavioral health challenges, there are immense societal ripple effects: long-term, prevention programs can reduce rates of child abuse and neglect, decrease violence and crime, and lead to increased employment and earnings.
Because of these outcomes, every dollar spent on prevention can yield a five- or even ten-fold return on investment by delivering cost savings across health care, education, criminal justice, and other systems.
In Oklahoma, prevention is underfunded and inadequate. Prevention programs exist, but they aren’t scaled to reach every child. Because of this, our state only reaches a fraction of the outcomes it could realize through a robust prevention strategy.
In this primer on prevention in Oklahoma, we outline why and how prevention works, when it is most effective, and what Oklahoma can do to maximize the potential of primary prevention.
Key takeaways
- Far more funding goes to treating mental illness and substance use than to upstream approaches that can prevent these problems from developing. The state mental health agency only allocates about 2.4% of its budget on prevention. Of that, only a fraction is spent on programming designed to prevent mental, emotional, and behavioral problems.
- Primary prevention works by reducing risk factors for developing mental health and substance use problems and shoring up protective factors that strengthen connection and build resilience in young people. For example, we could see 44% fewer cases of depression in adulthood by reducing adverse childhood experiences (ACEs).
- Oklahoma’s approach to prevention is largely siloed: agencies with similar goals operate their prevention initiatives in isolation. A unified prevention strategy led by a statewide prevention council could help funding go further and allow Oklahoma to reach every child with resources to prevent future behavioral health problems.
The cost benefits of investing in prevention
Cost–benefit analyses show that every dollar invested in primary prevention can yield many times its value in avoided costs related to treatment for mental health and substance use disorders, medical care, productivity losses, and the criminal legal system.
Universal, evidence‑based prevention programs generate returns that exceed their initial investments by reducing downstream costs in health care, education, child welfare, and the justice system.
Despite the cost effectiveness and proven outcomes of prevention, the vast majority of behavioral health funding goes to treatment for mental health and substance use disorders and other costs associated with these problems.
One study on substance use found that for every $100 spent on substance use and addiction in Oklahoma, only forty cents was invested in prevention, with the rest going toward addressing consequences.
Cost-benefit calculator
See what Oklahoma could achieve with the right investment in prevention.
The evidence for early, universal prevention
Over forty years of research demonstrates that behavioral health problems are preventable. Consistent evidence shows that problems such as anxiety, depression, and substance use can be reduced, delayed, or prevented using well-designed prevention programs.
For example, universal school-based strategies have been shown to reduce anxiety and equip students with self-management, social, and drug-resistance skills that help prevent adolescent tobacco use, alcohol use, binge drinking, and marijuana use. Family-based programs similarly reduce symptoms of anxiety and lower rates of substance use among adolescents.
Notably, prevention programs designed to prevent anxiety, substance use, and delinquency also provide protection against depression.
By implementing prevention strategies with children and youth before issues emerge, Oklahoma can avoid the social, emotional, and economic consequences associated with untreated behavioral health conditions.
The case for early prevention
Early prevention is crucial, because mental, emotional, and behavioral problems often develop early in a person’s life.
Half of chronic mental health conditions begin by age 14, and 75% by age 24.
Youth who begin using nicotine, alcohol, or other drugs before age 15 are 6.5 times as likely to develop a substance use disorder as those who delay use until age 21 or older.
Primary or early prevention is intended to reduce or altogether avoid risk factors that lead to behavioral health problems, so these challenges are prevented before they ever start.
Behavioral health problems depression, anxiety, and substance use have significant impacts on individuals’ and communities’ wellbeing and quality of life. When left untreated, these issues compound over time — and lead to significant costs for families, employers, communities, and public systems.
The case for universal prevention: The prevention paradox
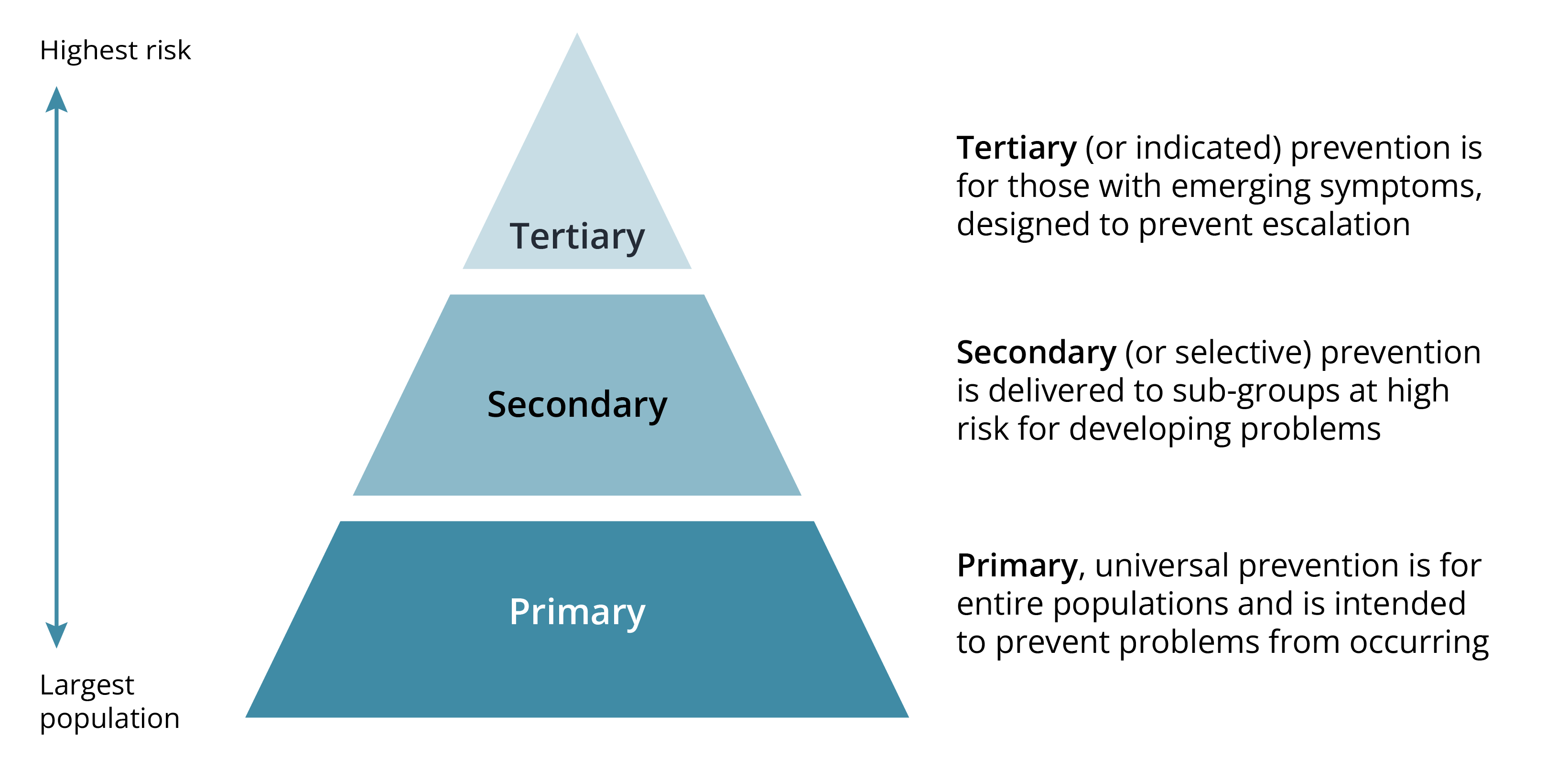
Primary prevention strategies are designed to be applied early but also applied universally — they are meant to build protection for entire communities, not just specific individuals or groups at higher risk.
Unlike selective approaches — which are only delivered to those at high risk and indicated approaches that target those with emerging symptoms — primary prevention approaches are wide-reaching, proactive, and meant to protect the development of behavioral health problems.
Primary, secondary, and tertiary prevention
Universal primary prevention goes against the traditional belief that interventions are best when focused on people at highest risk. But universal strategies produce the greatest total benefit because of what’s called the prevention paradox.
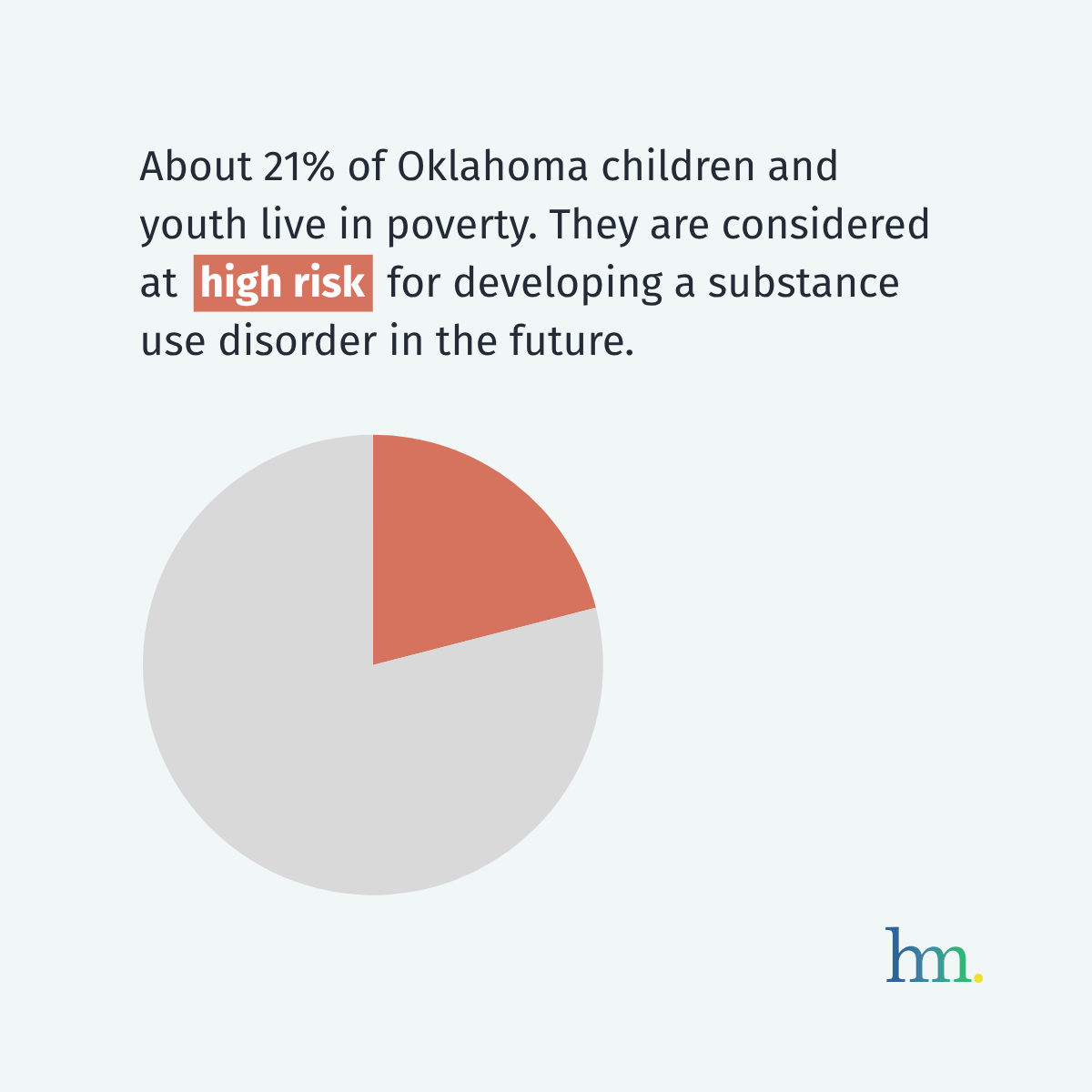
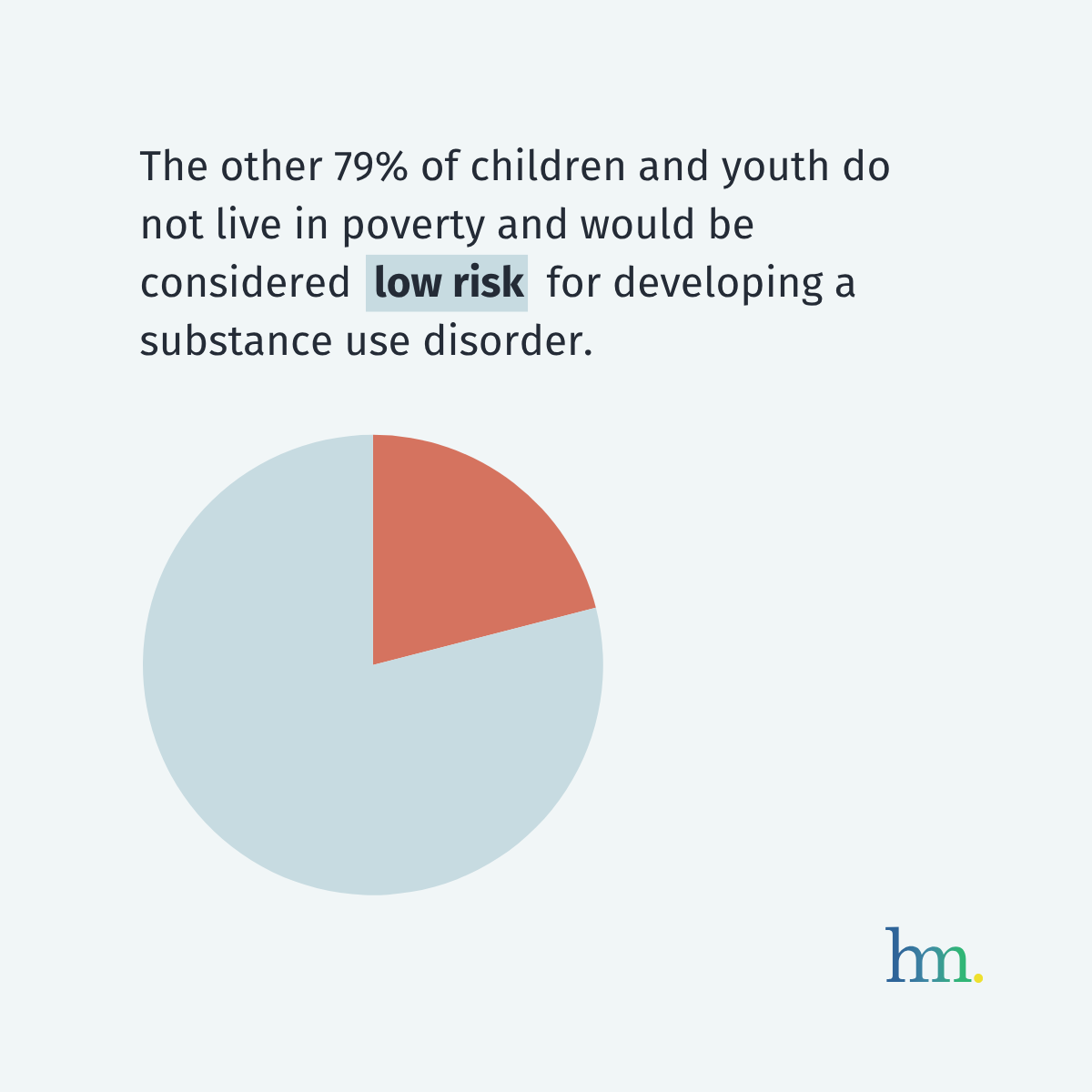
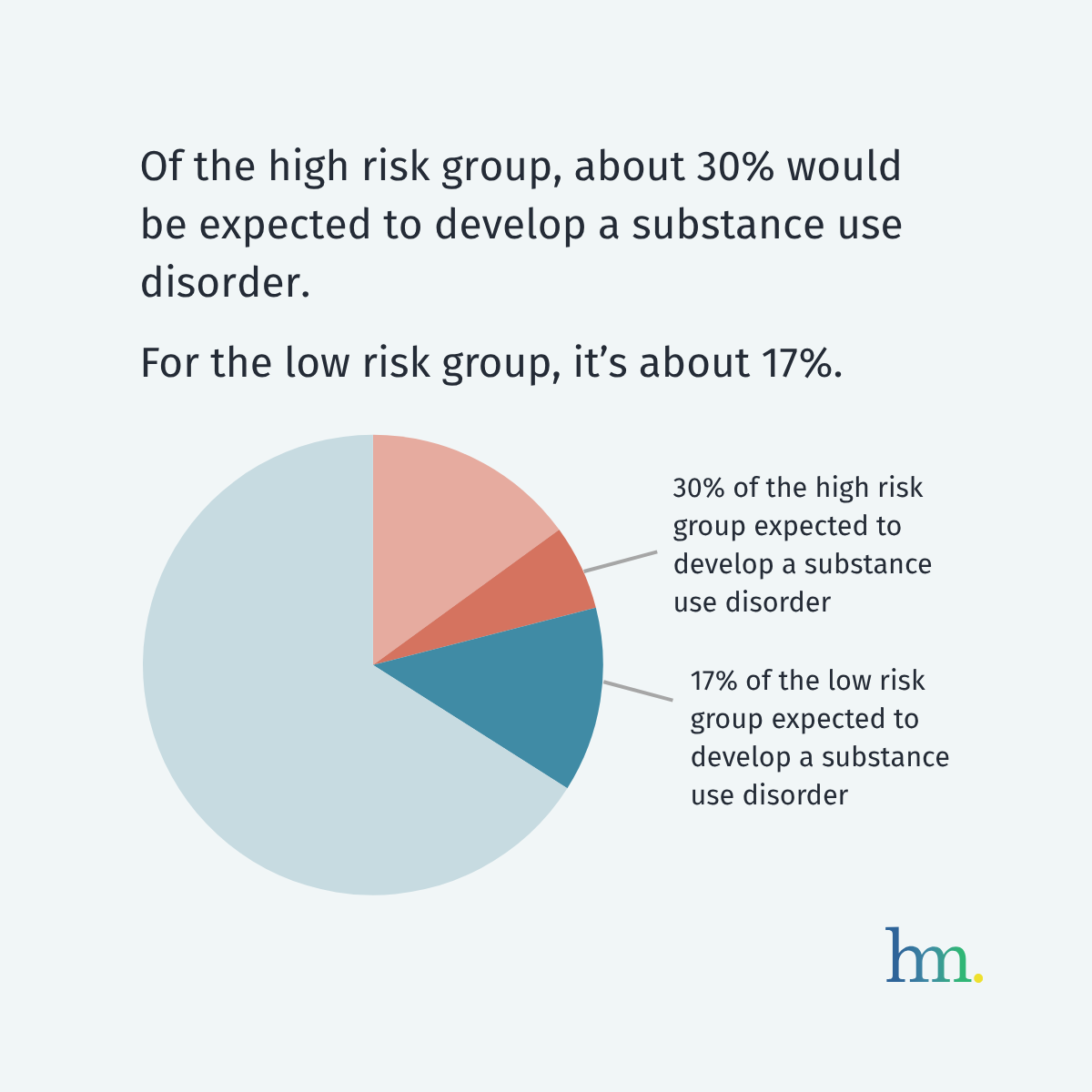
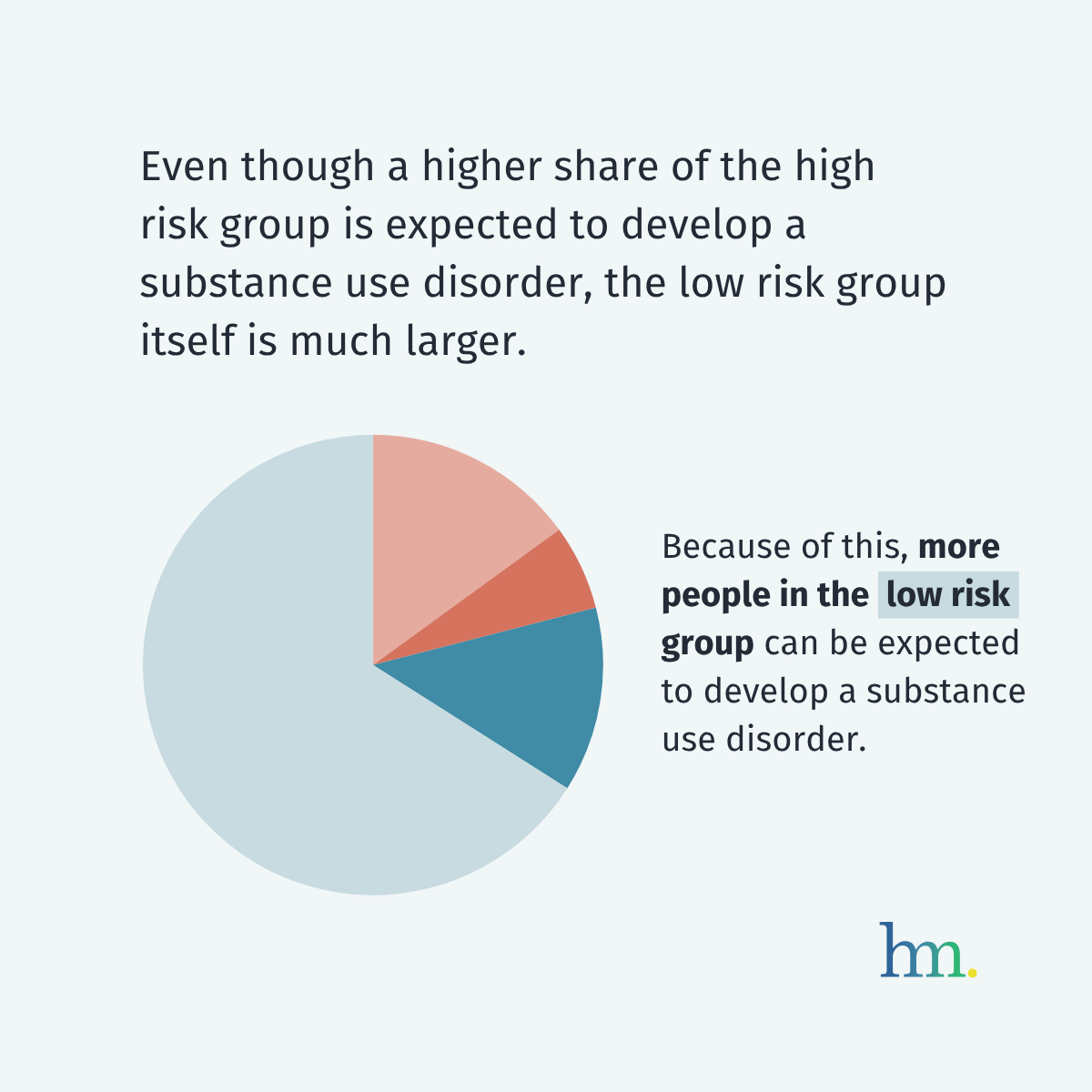
To understand the prevention paradox, consider two groups of people: One small group of people at high risk for developing behavioral health problems, and one much larger group of people at low risk. Even though a larger share of high-risk people will develop behavioral health problems compared to the low-risk group, the low-risk group is much larger, so more total cases of behavioral health problems will stem from the low-risk group.
In Oklahoma, the large number of people at low or moderate risk for behavioral health challenges collectively account for more mental, emotional, and behavioral health problems than the smaller group of people at high risk.
Because of this, population-wide prevention strategies have a greater overall impact than focusing only on intensive services for high‑risk people. By reaching children and youth across all risk levels, we can more effectively reduce the number of Oklahomans who go on to develop mental, emotional, and behavioral problems.
Illustrating the prevention paradox

Example Inputs
An example of the different input types.
How prevention works: Reducing risk factors, increasing protective factors
Throughout life, everyone will experience a combination of risk and protective factors that influence their mental health.
Prevention works by focusing efforts on reducing exposure to risk factors and bolstering important protective factors.
Risk factors are conditions or experiences that increase the likelihood a person will develop mental, emotional, and behavioral problems, while protective factors are the strengths, supports, and resources that promote resilience and healthy development. They go beyond individual circumstances — like poor self-esteem or emotional regulation — and can apply at the family, school, and community level.
Risk and protective factors, from individual to societal
- Poor self esteem
- Exposure to trauma, conflict, abuse, or neglect
- Perception of high substance use among peers
- Social isolation
- Lack of access to basic needs
- Biological and genetic vulnerability
- Poor emotional regulation
- Academic challenges
- Access to or unsafe storage of firearms or medications
- Positive self-esteem and sense of autonomy
- Emotional self-regulation and coping skills
- Substance use in family or home
- Family instability or changes in family structure
- Parental mental health challenges
- Peers who engage in unhealthy behaviors
- Lack of close peer relationships
- Aggressive peer behaviors
- Strong emotional support, guidance, belonging from family, peers, and adults
- Opportunities to develop problem-solving and communication skills
- Positive peer relationships and networks
- Stable, safe home environment and routines
- Access to nicotine, alcohol, and other substances
- Neighborhood violence
- Isolation at school and community
- Lack of mental health services
- Lack of youth programs, safe spaces to gather
- Poverty, economic hardship
- Engagement in school, extracurricular, and community activities
- Supportive and consistent relationships with trusted adults (mentors, teachers, caregivers)
- Exposure to substance advertising and use of substances in media portrayals
- Poor economic conditions, discrimination, and stigma
- Exposure to violence
- Inadequate social, public health services
- Punitive justice systems
- Policies that promote racial and health equality
- Food and housing security
- Health campaigns, counter advertising messages
- Enforcement of public health and safety laws and policies
The cumulative effects of risk and protective factors
Not all risk and protective factors carry equal weight.
Mental, emotional, and behavioral outcomes are shaped by both the amount and the strength of the risk and protective factors in a young person’s life.
For example, certain high‑impact risks, such as close friendships with peers who misuse substances, elevate the likelihood of problems more than lower‑impact risks, while some protective factors, like having a consistently supportive adult, can mitigate harm from multiple less impactful risks.
As the number of risk factors increases, the likelihood of problems rises. It is the cumulative burden, not any single factor, that most strongly predicts future mental, emotional, and behavioral problems.
Protective factors work similarly: Even when risks have accumulated, strong protections can help tip the balance toward healthy outcomes.
Visualizing risk and protective factors

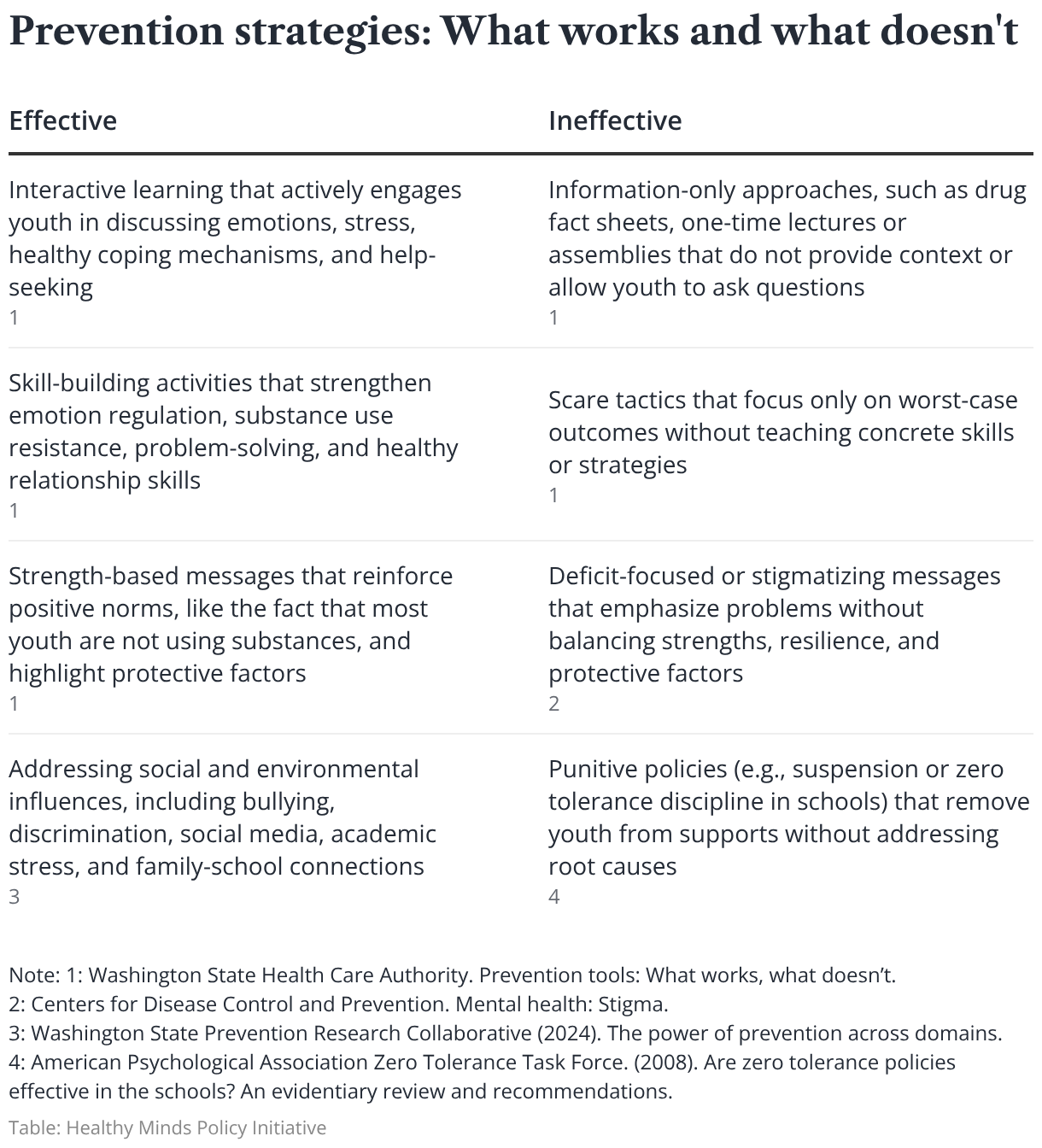
Effective prevention strategies
When selecting prevention strategies, communities should choose ones that have been proven to work. Because evidence-based strategies have rigorously researched — and repeatedly shown to improve outcomes — they are far more likely to produce real, positive change than untested ideas.
Well‑intentioned but untested prevention programs can be ineffective or even harmful, diverting energy and resources away from approaches that work.
Prevention in Oklahoma
Oklahoma’s primary prevention system is shaped by a mix of state and tribal government agencies and community-level organizations.
The Oklahoma Department of Mental Health and Substance Abuse Services (ODMHSAS) is the lead state agency charged with prevention of behavioral health problems among young people. ODMHSAS and other state agencies provide the core infrastructure, funding streams, and policy direction.
Day-to-day, Oklahoma’s prevention system relies on schools, tribes, health care providers, non-profit organizations, faith communities, and community-based coalitions to deliver services to youth across the state.
In this section, we highlight elements of Oklahoma’s existing prevention system — the degree to which programming prevention exists statewide, the agencies involved in prevention, and the workforce that supports these efforts — and offer opportunities that will help Oklahoma scale up prevention to meet residents’ needs today and for decades to come.
The scale of prevention efforts in Oklahoma
Oklahoma state agencies and tribes have shown their commitment to evidence-based prevention practices. But primary prevention programs administered by ODMHSAS and other agencies do not come close to reaching all children and youth across the state.
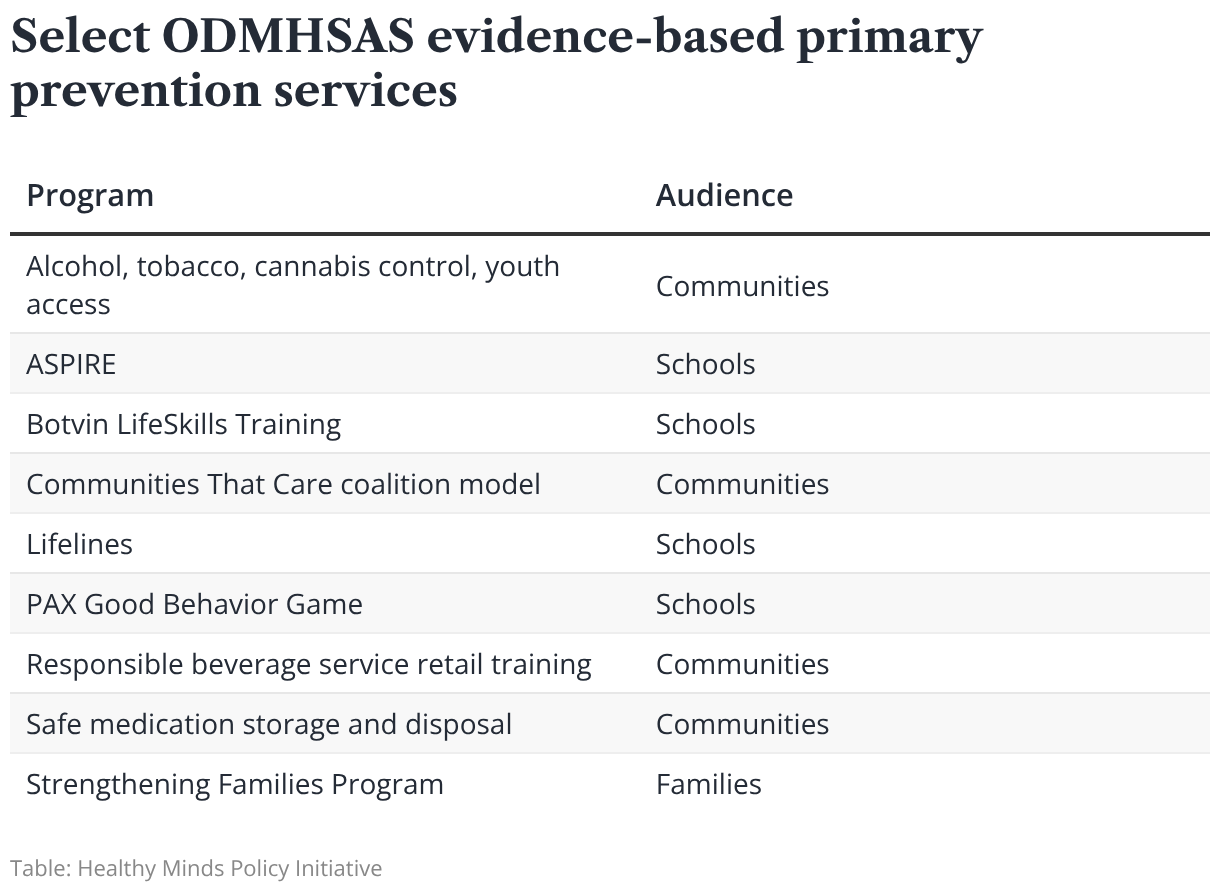
Instead, agencies typically award a limited number of contracts to entities that apply for funding, or they attempt to spread limited funds across the state to select geographic areas or on a county-by-county basis. In particular, ODMHSAS’ school-based primary prevention services reached only 23,116 students statewide in fiscal year 2025, a small fraction of Oklahoma students. See Appendix A for examples of ODMHSAS evidence-based primary prevention services.
In addition to direct services, policies at the city, county, and state levels play an important role in prevention in Oklahoma.
For example, youth access to alcohol is a well-established risk factor that can predict future substance use problems. State and local governments enforce the minimum drinking age of 21 through inspections and penalties, ultimately making it harder for youth to access alcohol and therefore reducing this risk factor.
Recent updates to alcohol related legislation have taken these efforts further by requiring retailer prevention training and strengthening penalties for adults who furnish alcohol to minors. During this time, the percentage of Oklahoma high school students reporting alcohol as easy to get decreased by 27% — with most 10th graders surveyed reporting alcohol as very hard to get.
Other examples of policy in Oklahoma that reduce risk factors for mental, emotional, and behavioral problems among youth include:
- Free pre K for 4-year-olds
- Bans on student cell phone use during the school day
- Suicide prevention training requirements for school staff
State spotlight
Utah lawmakers passed laws in 2017 and 2020 to require schools to offer students an evidence-based prevention curriculum, funded through alcohol tax revenue. The law resulted in statewide implementation of Botvin LifeSkills Training, ensuring that all students receive consistent, skills-based instruction in decision-making, emotional regulation, and substance use prevention.
New Jersey is rolling out Family Connects, a voluntary program that offers free, universal nurse home visits to all families in the state with newborns soon after birth. These visits include health checks for the baby and parent, support for feeding and newborn care, and connections to community resources to improve health, reduce stress, and promote family wellbeing. The program is supported through a coordinated mix of state dollars, philanthropic contributions, and other public funding sources.
The State Department of Health funds nurse home visitation in Oklahoma, but the program has eligibility and funding limits so not all families with new babies can be served.
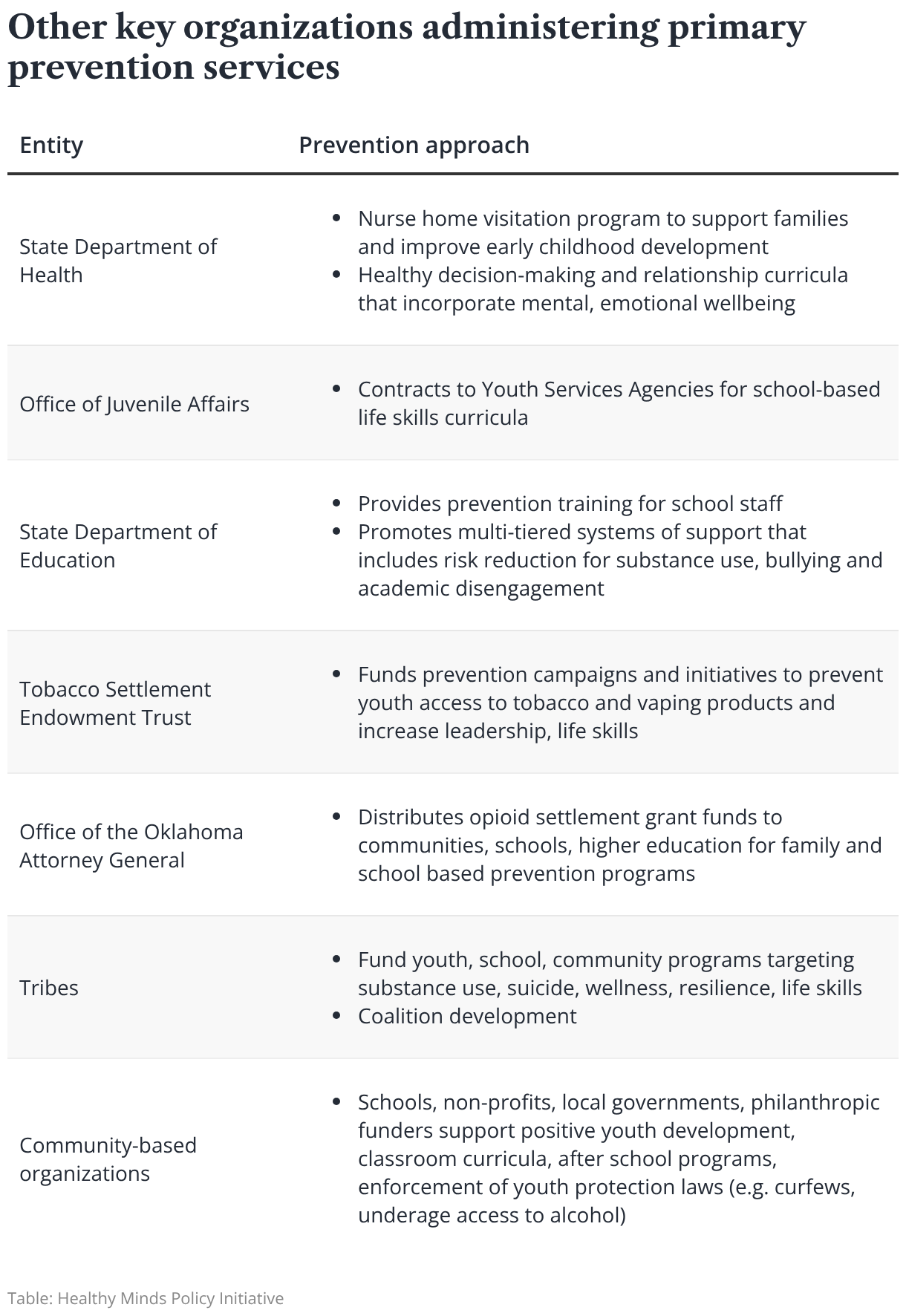
Decision-makers and agencies involved in prevention
ODMHSAS is the lead state agency charged with prevention of behavioral health problems among young people. Guided by an internal prevention strategic plan, ODMHSAS administers federal grants and state-appropriated prevention funds and provides technical support to workplaces, schools, health care settings, and faith communities.
In state fiscal year 2026, the agency funded 37 organizations to provide various levels of prevention services, not all focused on primary prevention. The agency supports a network of 51 community and campus-based prevention coalitions across the state made up of residents, youth, schools, colleges, faith partners, and organizational leaders. Contracted prevention agencies develop and support the coalitions and are charged with assessing local needs, building prevention capacity in the community, developing strategic plans, supporting the implementation of prevention services, and evaluating results.
Other state agencies administer prevention programs to further support healthy family functioning, expand school-based efforts, and strengthen community-led efforts. See Appendix B for more information about each agency and organization’s role in prevention.
Even when these programs do not primarily target mental health or substance use prevention outcomes, they address risk and protective factors — such as family violence, early trauma, school disengagement, and justice system involvement — that strongly influence the development of mental, emotional, and behavioral disorders in young people.
How prevention is funded
Funding for prevention works differently than for other health care services.
Public and private health insurers pay for much of the cost of treating mental, emotional, or behavioral disorders. Clinical providers deliver these services and are reimbursed for them by the insurer.
But in general, services to prevent these kinds of disorders are not reimbursable. Clinical providers can be reimbursed for problem identification or early intervention and treatment services, but universal primary prevention services provided before the development of a mental, emotional, and behavioral disorder are not covered in the same way.
Because of this, primary prevention in Oklahoma is funded through a mix of federal, state, and local funding streams. This includes:
- federal formula and discretionary grants
- alcohol sales taxes
- cannabis-related revenues
- state appropriations
- tobacco and opioid settlement funds, and
- contributions from charitable foundations
The majority of these funds are administered by state agencies and tribal entities, while some are distributed directly to local agencies and community-based organizations.
But prevention funding in Oklahoma has fallen to new lows, lagging both inflation and recent increases, according to state budget performance reports.
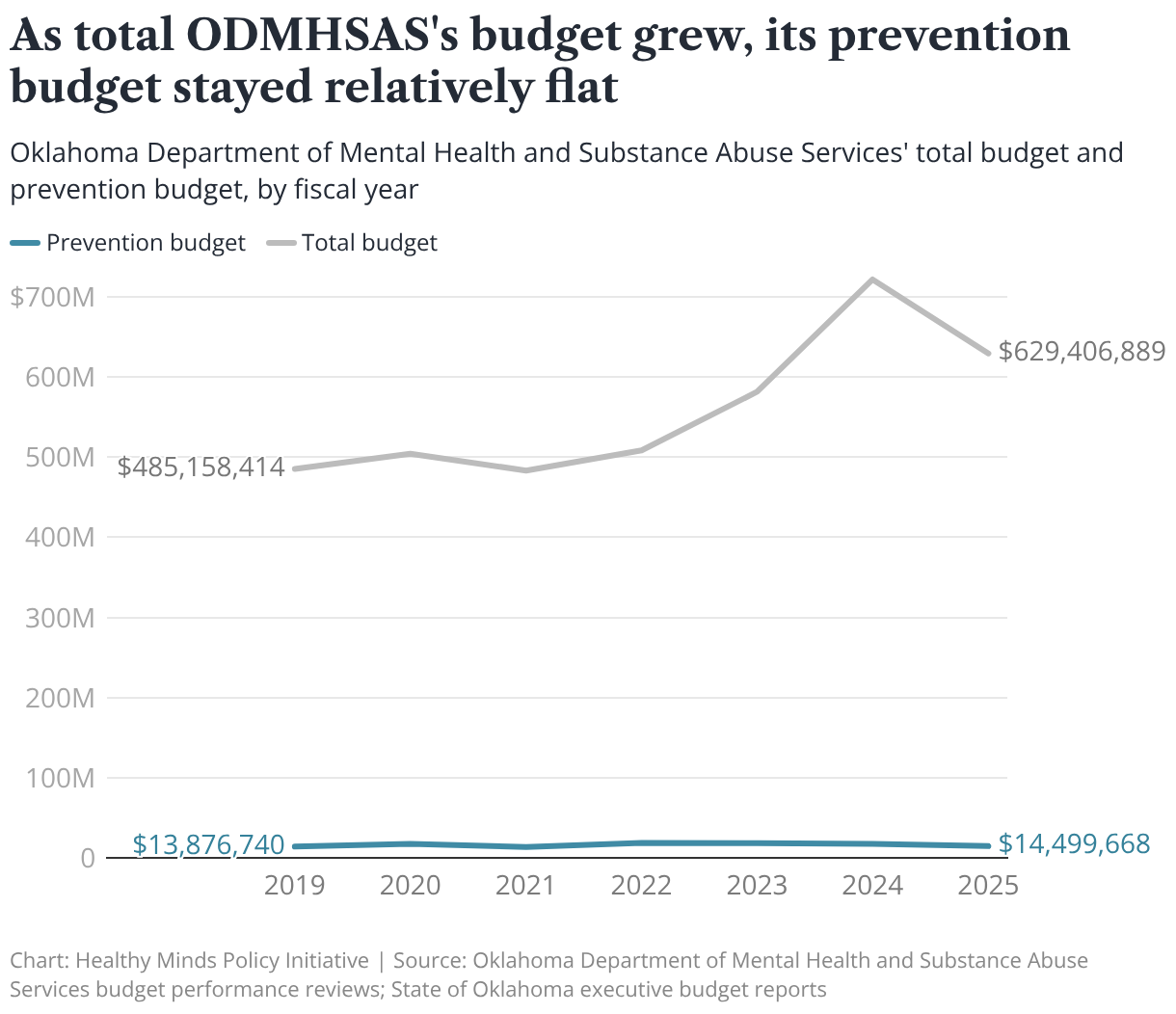
ODMHSAS spends an estimated $4.21 per Oklahoma resident on prevention, out of a total of $176.24 per resident in overall departmental spending. That is only 2.4% of ODMHSAS’ total budget allocated to prevention.
During the current fiscal year, 2026, ODMHSAS prevention funding dropped further to $12.7 million, a 30% decline since fiscal year 2022, and a new low in recent history. At the same time, the agency’s total budget grew by roughly 29.7%, with increases in fiscal year 2023–2024 followed by a decline in fiscal year 2025.
Of the fraction of the department’s budget spent on prevention, only about two-thirds is set aside for prevention support contracts and other spending related to preventing mental, emotional, and behavioral health problems.
The other third of the agency’s prevention budget is spent on early intervention, integrated behavioral health care, and crisis response services.
Breaking down Oklahoma’s federal funding for prevention
Most of ODMHSAS’s prevention budget comes from federal funding — about 77% in fiscal year 2024 — with the rest from state appropriations and revolving funds.
Much of the federal funding comes to ODMHSAS through the Substance Use Prevention and Treatment Block Grant provided to all U.S. states and territories by the Substance Abuse and Mental Health Services Administration (SAMHSA). This is a non-competitive “formula” grant, which means states and territories receive a calculated amount of funding based on several factors, including their population at risk and costs of services.
The block grant covers prevention and treatment for substance use and requires states to dedicate at least 20% of their allocation to primary prevention services.
Oklahoma currently allocates only the minimum required 20% of its block grant to primary prevention. Other states invest more than the minimum, especially as Medicaid expansion has freed up block grant dollars by shifting more treatment costs to Medicaid.
ODMHSAS also budgets 20% of its State Opioid Response grant, a federal formula grant, to prevention. However, the department has no written policy in place to ensure this practice continues.
Oklahoma also benefits from SAMHSA “discretionary” grants, which are competitive awards to states, tribal nations, and organizations. Over the past seven years, Oklahoma entities received over $62 million in discretionary funding from the SAMHSA Center for Substance Abuse Prevention.
ODMHSAS is the largest recipient, followed by Cherokee Nation, Southern Plains Tribal Health Board Foundation, and the University of Oklahoma. Oklahoma tribes significantly contribute to the state’s overall investment in prevention services — more than $7.5 million in competitive primary prevention grants from SAMHSA has been awarded to Oklahoma tribal governments and tribal serving entities over the past three years.
Opportunity: An integrated prevention governance structure and unified strategy
Oklahoma has the foundation for wide-scale primary prevention initiatives, but its approach to prevention is largely siloed. Oklahoma must scale its existing prevention efforts to reach every child in Oklahoma, but this won’t be possible unless agencies and organizations work together.
Without a unified prevention agenda or coordinated strategy, agencies and organizations generally operate independently of each other, even when they have common goals.
For example, today, three state agencies support varying degrees of Botvin LifeSkills Training, but they lack formal coordination of funding, training and other supports for schools. Instead, communities apply for a limited number of contracts to utilize the program and work directly with each state funder to implement the program.
If Oklahoma developed a coordinated, integrated prevention governance structure, the state could better use its limited prevention dollars and align strategies toward common goals. Ideally, state agencies would work together, guided by a state-level coordinating council, to braid resources and select evidence-based strategies that are most needed.
An accountable prevention council would coordinate across mental health, substance use, education, health, child welfare, justice systems, researchers, private funders, and other sectors to reduce fragmentation and align prevention efforts toward common outcomes.
The group could also adopt a standardized definition of primary prevention, design a coordinated strategic plan, issue guidance and technical assistance, reduce duplication and conflicting requirements, and recommend policy and regulatory changes. And a state prevention council could be charged with identifying ways to coordinate existing funding and generate new resources for primary prevention, which could include:
- coordinated agency state appropriation budget requests
- braided budgets aligned with shared priorities using existing funding sources
- cross agency commitments to increase prevention budget investments (e.g. ODMHSAS block and formula grants budget at least 30% for primary prevention)
- managed care funded specialty programs or healthy community incentives
- municipal, county health impact bonds
- wellness trusts funded by public, private resources
- dual impact policies that both prevent mental, emotional and behavioral problems and increase revenue such as excise taxes on alcohol, tobacco and cannabis products reinvested in prevention
- health insurance billing approaches that maximize services to covered patients by serving the child’s whole classroom or family (e.g. well-child pediatric visits that integrate family primary prevention skill building)
Today, groups that once coordinated prevention strategies no longer convene. For example, ODMHSAS, OSDH and TSET previously facilitated the Public Health Academy of Oklahoma, a cross-agency committee to more efficiently coordinate prevention training and other processes among local prevention organizations receiving funding from the agencies.
ODMHSAS also previously spearheaded a state prevention advisory body that included governmental agencies, non-profits, universities and other key prevention workforce to develop a state-level prevention plan and better align scant resources.
State spotlight
The state of Washington established the State Prevention Enhancement (SPE) Policy Consortium in 2011, a statewide policy and planning body made up of representatives from over 20 state and tribal agencies and organizations that collaborate to guide prevention. It still leads state level strategic planning, sets shared priorities, and coordinates a unified state strategy with joint investment in the plan. The consortium oversees workgroups on prevention topics like opioids, underage drinking and cannabis use, problem gambling, tobacco and vape product use, and mental health promotion that directly shape operations.
Oklahoma’s prevention workforce
Oklahoma’s prevention workforce includes leaders and specialists who develop strategic plans, coordinate coalitions, conduct community needs assessments, and manage funding.
It also includes frontline implementers who deliver curricula and advance policy strategies, as well as trainers and technical assistance providers who support prevention professionals on core competencies and fidelity to evidence‑based practices.
For these prevention professionals, the most widely preferred credential is the Certified Prevention Specialist. Many employers require it or strongly prefer it, and certification is administered through the Oklahoma Drug and Alcohol Professional Counselor Association and aligns with international standards. It is increasingly regarded as the minimum professional standard for prevention specialists.
But the career pathway for prevention specialists is underdeveloped. Job titles, salaries, and advancement opportunities vary widely; many positions are tied to grant cycles rather than permanent workforce structures. Outreach and recruitment are similarly decentralized, often dependent on individual employers or regional entities.
Oklahoma also lacks robust data sources to quantify the size and capacity of its prevention workforce. The state certification organization reports roughly 50 Certified Prevention Specialists and 10 Associate Prevention Specialists (an entry-level prevention credential), while the international certification body reports 27 Certified Prevention Specialists in the state.
Other core parts of the prevention workforce include people who do not primarily identify as prevention professionals also deliver mental, emotional and behavioral prevention services. These include trained youth leaders, school staff implementing evidence‑based programs, social workers, public health educators, primary care and behavioral health providers, home visitors and early childhood professionals, and faith and community leaders working to strengthen protective factors.
Prevention data
In addition to lacking workforce data, Oklahoma lacks a unified system to collect, track, and report the reach and outcomes of prevention services across the state. Robust data is essential for assessing prevention needs, planning, and evaluation.
ODMHSAS does collect and track some prevention data, including the results of the Oklahoma Prevention Needs Assessment (OPNA), a statewide biennial survey of students in grades 6, 8, 10, and 12. The survey is voluntary and requires parent or guardian consent, and it tracks youth substance use, mental health, violence, and related risk and protective factors to guide local prevention planning.
The department also collects prevention service, fiscal, and basic outcomes data from grantees and subrecipients of prevention funding. But despite these data collection efforts, Oklahoma does not yet have a unified system that consistently tracks and reports prevention services, reach, and outcomes across diverse funding streams.
Without standardized methods, agencies often rely on various grant reports, surveys, or local spreadsheets, which makes it difficult to aggregate data across funding sources and programs, compare outcomes, or follow trends over time. Different funders and systems typically use their own definitions, indicators, and reporting timelines, so data are inconsistent and cannot easily be combined into a statewide picture.
Opportunity: Expand prevention workforce pathways and data collection
An Oklahoma prevention council could build the infrastructure needed for a strong and sustained prevention workforce and the data needed to evaluate prevention needs and outcomes across the state.
The council would assess workforce needs and should develop a primary prevention workforce plan, spanning sectors including public health, education, child welfare, behavioral health, health care, and community-based organizations.
This would include expanded training for both dedicated prevention professionals and prevention-adjacent staff in other sectors and formalizing a career pathway for prevention service providers by defining clear roles, competencies, and salary bands. The state should also expand practicum and apprenticeship pathways.
Oklahoma should stabilize prevention workforce funding by moving beyond short-term grants toward braided or sustained financing models that support permanent prevention positions.
Similarly, Oklahoma’s lack of an integrated prevention data system results in fragmented information and limits the state’s ability to assess overall impact.
To fix this, an Oklahoma prevention council should identify a core set of prevention indicators and data collection requirements and establish shared reporting across state agencies. The council and state agencies would use the data to assess prevention needs, the reach of prevention services, outcomes from primary prevention strategies, and identify gaps and opportunities for improving the quality of prevention programs.
The bottom line
Investing in prevention is investing in Oklahoma’s future. Through prevention, Oklahoma can protect the mental and behavioral health of children and youth in all 77 counties — and achieve the long-term benefits of a healthier state.
Oklahoma must shift from a siloed, agency-by-agency approach to a unified, coordinated prevention strategy. It must move beyond short-term, piecemeal grant opportunities and instead find sustainable funding models for permanent prevention efforts and their necessary workforce.
And finally, to achieve the maximum benefits of a state where fewer people develop behavioral health challenges, Oklahoma’s prevention strategy must be applied universally and scaled to reach every young person across the state.
Appendices
Appendix A
Appendix B