
Barriers to care for people with co-occurring mental health disorders and intellectual and developmental disabilities
People with intellectual and developmental disabilities, or IDD, are at higher risk of experiencing behavioral health conditions such as depression, anxiety, and bipolar disorder. In fact, research has shown that between 39 and 52% of people with IDD — one to two million people nationwide — have a co-occurring psychiatric condition.
But because of stigma, a lack of training among health care professionals, and inadequate, disconnected community supports, people with IDD and co-occurring mental health challenges face obstacles that make it difficult to access the behavioral health care they need.
For many people with IDD — which can include Down syndrome, autism spectrum disorders, hearing or vision impairment, and Huntington’s disease, among others — health care providers focus on treating their physical health and cognitive needs. Unfortunately, behavioral health challenges often go overlooked and unaddressed in people with IDD.
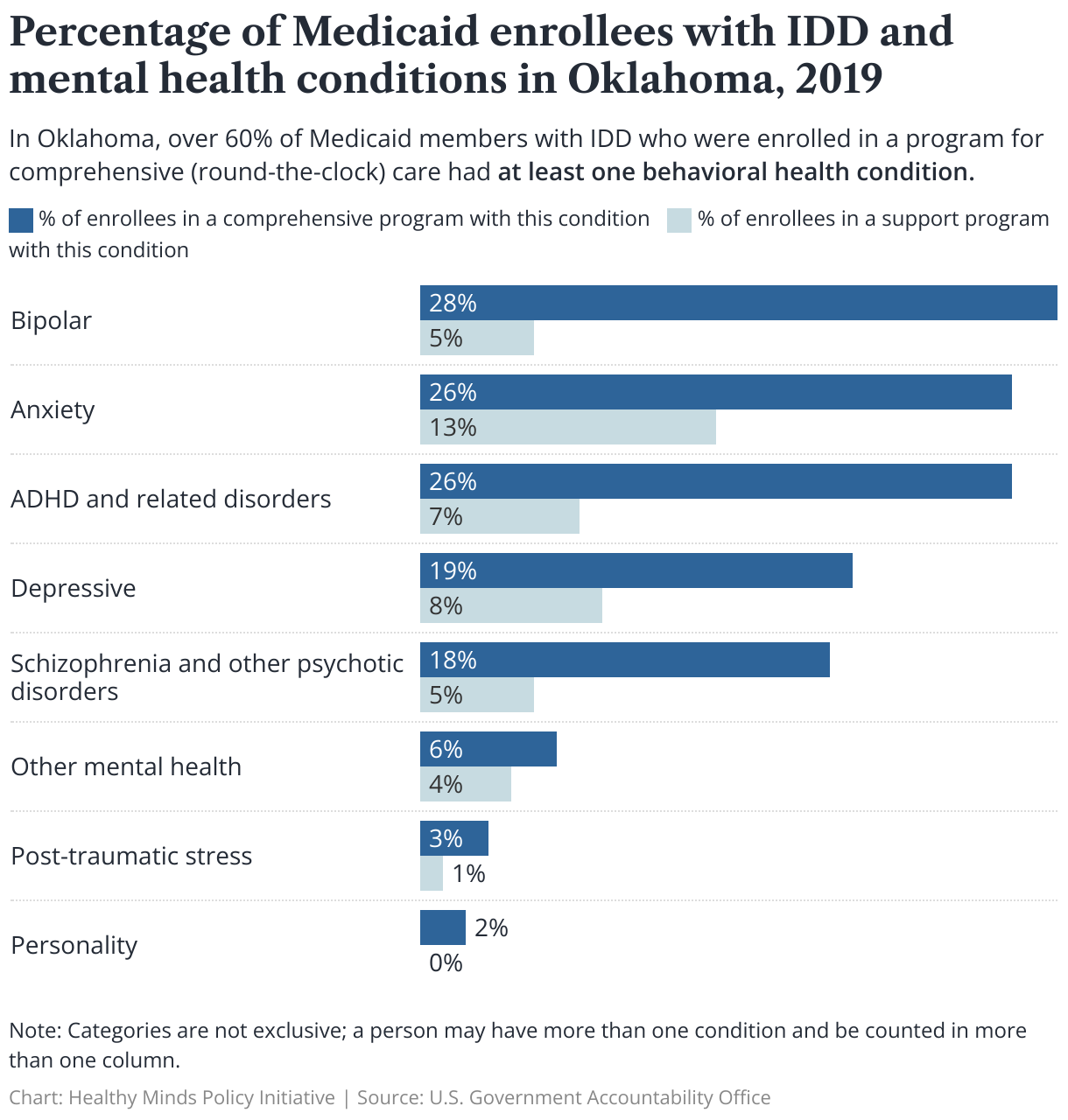
In Oklahoma, over 25% of Medicaid members enrolled in a home- and community-based services (HCBS) program aimed at supporting people with IDD to live in their own or a family home had at least one behavioral health condition, according to a Government Accountability Office report. Moreover, more than 60% of Medicaid members enrolled in a HCBS program that provides around-the-clock care and residential services for people with IDD had at least one behavioral health condition.
While we know many people with IDD have a co-occurring psychiatric condition, it can be difficult to precisely quantify this population because of inconsistent data collection. Estimates are believed to undercount the actual prevalence of mental health conditions among people with IDD.
In this analysis, we examine barriers to care for people with IDD and co-occurring behavioral health conditions in Oklahoma. In a future publication, we will explore solutions and highlight initiatives already underway to alleviate these obstacles.
Key takeaways
- Stigmatizing attitudes toward people with IDD from the public and health care professionals is a critical barrier to accessing appropriate mental health care. Misconceptions about whether people with IDD can benefit from therapy — as well as strict, discriminatory treatment admission requirements that rely on I.Q. score — prevent people with IDD from getting the care they need.
- Health care providers lack training and expertise in working with people with IDD, which can lead to behavioral health challenges being overlooked or even misdiagnosed.
- Oklahomans with IDD and their caregivers often encounter inadequate, disconnected behavioral health care systems. A lack of community-based crisis services and barriers to accessing inpatient care lead to overreliance on emergency room visits for mental health crises.
Identifying barriers to behavioral health care
People with IDD often struggle to access appropriate mental health treatment. In a national study, local IDD agencies and Medicaid staff reported several barriers to care for this population: a shortage of mental health providers who are trained and comfortable working with people with IDD, insufficient behavioral health supports, and a lack of collaboration among systems. People with IDD and co-occurring mental health conditions may also face stigma and difficulties in coordination and communication between service providers and families or caregivers.
Stigma and discrimination
Stigma associated with IDD can manifest in many ways, from exclusion to biased attitudes and unfair treatment. People with IDD often experience stigma socially and in health care systems, which can lead to isolation, loneliness, low self-esteem, and even increased symptoms of depression and anxiety and negative self-evaluations.
Access to mental health care, including therapeutic intervention and counseling services, is crucial for people with IDD who also have mental health challenges. However, some facilities and practices have strict admission requirements that exclude individuals with I.Q. scores below 70, leading to discrimination.
A person’s I.Q. score or intelligence level alone cannot determine whether they may benefit from therapy and other types of behavioral health care, despite the misconception that people with IDD do not benefit from therapeutic interventions. Exclusion from services based solely on I.Q. scores can prevent individuals with IDD and mental health problems from receiving the care they need.
When tailored to an individual’s unique needs and abilities, psychotherapy can be effective for people with IDD. For example, therapy can be more effective for people with IDD by adjusting the language, frequency, and duration of sessions, coordinating with other professionals and organizations involved in the person’s care, providing positive feedback, and being flexible enough to modify the therapeutic approach to meet the individual's needs. Talking Mats® is one example of an evidence-based practice clinicians can use, involving an interactive set of picture communication symbols to engage with patients who may struggle to communicate verbally.
People with IDD do not only face discrimination in behavioral health settings: doctors in primary care practices and specializations often turn away individuals with disabilities. A study conducted by medical schools in Illinois and Massachusetts revealed that doctors often tell patients with disabilities that they would require specialized care or that they are not taking new patients, and others explicitly expressed bias toward this population. Another study by the same group found that only 56% of doctors welcome patients with disabilities into their practices.
This failed approach needs to change, and providers — as well as society at large — must learn to see people with IDD through a lens of strength and capability rather than limitation and incapability. Breaking down stigma and structural discrimination is an important part of ensuring equitable access to medical and mental health care for individuals with dual diagnoses of IDD and mental health conditions.
Lack of experience, training among providers
People with IDD and their caregivers expect health care providers to be knowledgeable, communicate effectively, and dedicate sufficient time to address their needs. However, some providers fall short of these expectations. People with IDD frequently encounter mental health professionals who lack adequate understanding of IDD and receive insufficient training on addressing their needs and available treatment and support options.
In one study, only 41% of doctors were confident they could provide patients with disabilities with similar quality care as other patients, and more than a third of doctors also reported having little or no knowledge of their legal obligations under the Americans with Disabilities Act.
Providers’ lack of understanding of the rights afforded to people under the ADA could lead to unintentional discrimination. For example, a therapist may not provide reasonable accommodations such as adjusting the session length or providing accessible therapy spaces. This can result in unequal access to mental health care, which is a violation of the ADA.
Some Oklahoma families have reported instances in which facilities failed to fulfill their obligation to assess and treat individuals regardless of disability. In one case, an Oklahoma advocate interviewed for this paper reported that a person with autism was in a severe mental health crisis and was actively suicidal. The person went to a mental health facility for help but was not allowed to enter and instead was assessed in the parking lot. Through the assessment, the person met criteria for admission but was denied care, as staff at the facility claimed they couldn’t handle treating the person because of their level of autism.
Incidents like these underscore the importance of mental health professionals being educated on their legal obligations to ensure they provide equitable care to all patients, including those with IDD.
Furthermore, clinicians face challenges in identifying emotional or psychiatric disorders in individuals with IDD due to a lack of experience in working with this population, communication barriers, and a tendency to overlook or underestimate signs of psychiatric issues and attribute them to the individual's disability. This can lead to misdiagnosis and the prescription of psychiatric medications such as antipsychotics, antidepressants, and mood stabilizers as the primary treatment. Non-medication supports in IDD, such as referrals to community supports, behavioral and educational interventions, or psychotherapy, are underused despite being an ideal form of intervention before trying medication.
Our state is no exception to these challenges. Some clinicians have reported that mental health providers in Oklahoma do not have sufficient training to address the needs of patients with IDD. This includes interacting with them and providing diagnostic and treatment planning and services. Additionally, experts in the field may not consider it their responsibility to provide basic mental health care to this population.
Providers’ lack of training is often on display during discharges too. Oklahoma families have reported that their loved ones may be discharged prematurely because the program disapproves of their behavior (related to their diagnosis) or because the discharge plans are poorly designed and lack comprehensive care for people with IDD. When working with patients with IDD, staff fail to consider appropriate placements outside of institutions or at a higher level of care and do not involve guardians or caretakers, who should be actively engaged in the discharge planning and service provision.
Others shared that a lack of community-based services forces parents to check their children into the emergency room for help. Community-based services can include a broad range of supportive resources and interventions delivered in the community, such as outpatient care, medication management, crisis services, case management, and intensive community treatment. Without access to these kinds of supports, families often keep children with IDD at home, where caregivers may lack the resources to adequately offer behavioral health support to the child.
Oklahoma also has significant behavioral health workforce shortages, which only compounds a lack of clinicians trained to work with people with IDD. This population often requires specialized care and support from highly trained and experienced professionals. However, due to workforce shortages, many of these individuals cannot access experienced providers to address the care they need, which can negatively impact their health and well-being.
Research consistently highlights the need for more training and experience for professionals when working with individuals who have IDD. Psychiatrists, psychologists, and primary care physicians receive little or no exposure to IDD in their training, highlighting a clear need for more opportunities for professionals across fields to specialize in care for people with IDD.
The American Academy of Developmental Medicine and Dentistry recognized a deficiency in IDD training and created a funding stream in 2009 to remove financial obstacles to integrating IDD education into the curricula of all U.S. medical schools. But as of 2023, only 15% of American medical schools had used these grants.
Inadequate treatment and supports
The challenges people with co-occurring IDD and mental health challenges and their families face are complex and multi-faceted. Insufficient and uncoordinated services, a lack of understanding and stigma, a lack of collaboration among different agencies, and poor communication create significant burdens on families and patients. The gaps in mental health system further compound the problem by the lack of crisis, night, and weekend services, limited choices of services and providers, and inadequate specialized training for providers.
For instance, an individual with dual diagnoses may need behavioral support from the IDD sector and therapy from the mental health sector. However, the individual may not receive both services and supports to address their needs due to a lack of coordination between these two sectors. Therefore, it is crucial to have effective coordination and collaboration among healthcare systems and agencies to provide comprehensive, accessible, and high-quality services to individuals with dual diagnoses and their families.
A lack of community-based mental health services for people with IDD may also force this population to rely on emergency departments during a crisis, which can lead to disparities in access to mental health services. Inadequate preventive care and health promotion activities can ultimately result in a higher likelihood of hospitalization and lower quality of life for those with IDD and mental health conditions.
One study found that 74% of individuals with intellectual disabilities who went to the emergency department for mental health reasons had already visited the emergency department for mental health concerns at least once in the previous year. This suggests that emergency departments may not be fully addressing the mental health needs of patients with intellectual disabilities during their initial visit. This could be due to a lack of training, appropriate links to referrals, supports, and resources.
Families in Oklahoma seeking outpatient mental health care for children with IDD face limited options, often leading to a crisis that requires inpatient treatment. However, locating an inpatient facility equipped to handle individuals with IDD poses its own set of challenges.
Tulsa has the state-run Laura Dester Children’s Center, which can provide short-term treatment and stabilization services for children under 17 with IDD and mental health conditions who are also wards of the state. But there are no comparable facilities for children not in child welfare custody. As a result, these children may be sent to facilities out of state, creating significant challenges for families who lack the resources to visit them. This can also make reunification difficult.
Challenges for caregivers
Caregivers of individuals with IDD play a vital role in providing support and insights into their loved ones' medical histories and unique needs. However, they often face challenges in coordinating care for their loved ones and receiving support to take care of their own mental and physical health.
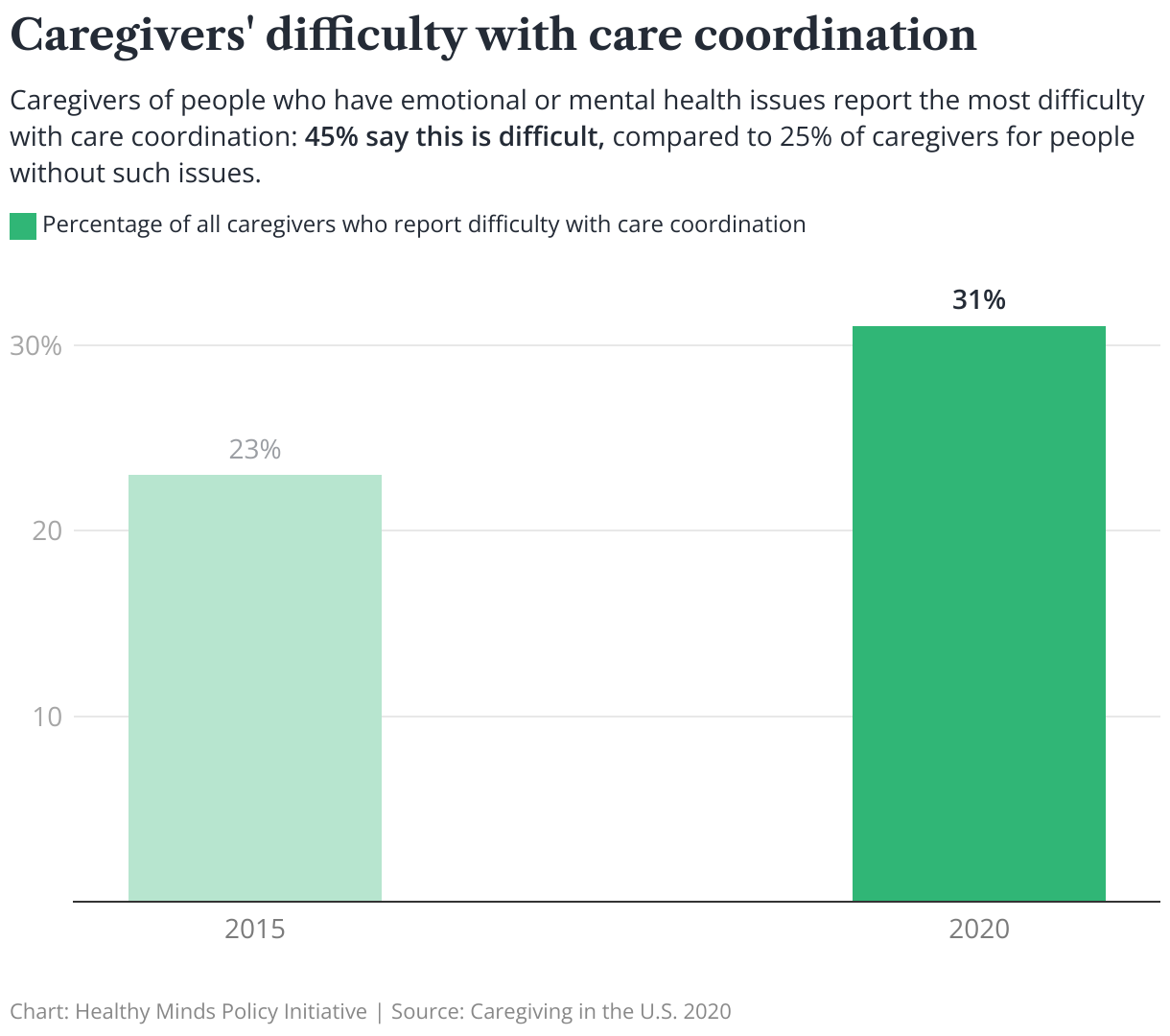
In a recent national survey, 31% of caregivers reported difficulty coordinating care across various providers, up from 23% in 2015. Caregivers of people with emotional or mental health issues reported the most difficulty with care coordination, with 45% reporting difficulties compared to 25% of those caring for recipients without such issues.
The demands of caregiving can also create high levels of stress. Research shows that caregivers and their families can benefit from adequate assistance, which can increase their well-being and quality of life. However, only 21% — or 1.54 million — out of the approximately 7.43 million people with IDD in 2018 were served by state IDD agencies. People not currently served by state IDD agencies may only come into contact with these systems during a crisis, such as the sudden death or decline in the health of a parent. This could lead to them receiving less desirable and more costly services.
To better support individuals with IDD and their aging caregivers, state Medicaid agencies and their partners can proactively plan for future needs. This can include building partnerships, providing engagement and navigation support, and planning for the future. States can also offer multiple services to support aging caregivers and individuals with IDD, such as respite, counseling, assistive technology, and specialized devices for maintaining independence at home. Respite care is a particularly crucial service that can provide temporary relief and help prevent caregiver burnout.
Overcoming obstacles
People with IDD face multiple, compounding barriers to accessing the appropriate mental health care for their needs, including stigma and a shortage of providers with experience and training in treating co-occurring IDD and mental health challenges. To overcome these obstacles, Oklahoma and other states must invest in early and continuing training for health care providers, better integrate and coordinate systems of care for people with IDD, and work to combat stigmatizing attitudes toward people with IDD.
