Supporting Oklahomans after incarceration through Medicaid
Each year, nearly 217,000 people are released from Oklahoma prisons and jails. The reentry period can be a vulnerable time, as people often must quickly find jobs, housing, health coverage and other community supports to survive.
In the two weeks after release from incarceration, a person is 40 times more likely to die of an opioid overdose, one study found. Formerly incarcerated people are also 10 times more likely to be homeless and twice as likely to die by suicide compared to the general population.
Supporting people released from incarceration is especially urgent in Oklahoma, where the prison population is rising again after declines in recent years. Oklahoma has among the highest incarceration rates in the nation — at any given time, about 34,000 people are held in Oklahoma’s county jails and state and federal prisons.
As incarceration rates have increased, jails and prisons have become de facto mental health facilities, despite lacking the appropriate programming and services to meet people’s mental health and substance use needs. In Oklahoma, the state Department of Corrections (DOC) estimates that 38% of the state’s prison population has symptoms of a serious mental illness, and this figure likely underestimates the prevalence of mental illness among incarcerated Oklahomans. For comparison, only about 5.5% of U.S. adults have a serious mental illness.
A policy dating back to Medicaid’s origin in the 1960s prevents the program from paying for health care provided to people incarcerated in jails and prisons. But some states, with federal approval from the Centers for Medicaid and Medicare Services (CMS), have begun using a new Medicaid strategy to offer limited health coverage to people nearing their release date, creating a safer and more supportive community reentry period by covering transitional case management, medication assisted treatment, and more.
In this analysis, we examine this Medicaid strategy — a Section 1115 reentry waiver — and its potential in Oklahoma, highlighting key components of programs approved in other states to support justice-involved people before their release from jail or prison.
Key takeaways
- Incarcerated people are especially vulnerable to physical and mental health challenges after being released, posing an urgent challenge for Oklahoma, which has among the nation’s highest incarceration rates.
- Currently, Medicaid is prohibited from paying for health care services in jails and prisons, but CMS has encouraged states to use a new Medicaid strategy to offer limited health coverage to incarcerated people nearing their release date.
- A lack of comprehensive data collection in jails and prisons is a barrier to identifying incarcerated people eligible for Medicaid.
- Oklahoma can join other states in using this new Medicaid strategy by amending its existing Section 1115 waiver to include the reentry population, which would offer health coverage through Medicaid for people being released from prisons and jails and create a smoother community reentry period.
Background: Oklahoma and the inmate exclusion policy
In Oklahoma, more than 1 million low-income residents have health coverage through SoonerCare, the state’s Medicaid program, which is managed by the Oklahoma Health Care Authority, or OHCA.
When Medicaid was established by Congress in 1965, the law included a provision that prevents the federal government from being responsible for health care costs in local jails and state prisons. The policy, often referred to as the “inmate exclusion policy,” applies to anyone being incarcerated overnight, including people awaiting trial and those who have been convicted. (Medicaid will pay, however, for an incarcerated individual’s health care costs when admitted to a medical facility for inpatient care overnight.)
Although many incarcerated people qualify for Medicaid, the inmate exclusion policy either terminates or suspends a person’s Medicaid coverage while incarcerated, depending on the state’s rules. In Oklahoma, incarcerated people are not disenrolled from SoonerCare; instead, an incarceration indicator is added to their account.
OHCA reported that 3,380 SoonerCare members are currently incarcerated as of July 2024, including 928 who are part of the Medicaid expansion population. However, these totals are likely a significant undercount, as the agency relies on individuals or their family members to call, go online, or visit the agency to self-report the member's incarcerated status. Without these voluntary updates, OHCA cannot identify whether a person is incarcerated, resulting in incomplete reporting.
For people incarcerated in Oklahoma prisons, OHCA works with the DOC to facilitate SoonerCare applications for people in prison. The partnership between the two agencies was established during implementation of Oklahoma’s Medicaid expansion, which took effect in 2021. Through the partnership, DOC staff can submit SoonerCare applications on a prisoner’s behalf about 30 days before they are set to be released. Once the person is released, and if they meet all eligibility requirements, they can activate their Medicaid coverage by contacting OHCA or a community partner. There is no processing time – their coverage can take effect the same day.
However, there is no similar process in county jails. County jails hold thousands of people each day, many of whom could be eligible for SoonerCare, but these facilities lack a data collection system to track basic information about people being held in jail, including whether they may qualify for SoonerCare.
House Bill 3848, by Rep. Meloyde Blancett (D-Tulsa) and Sen. Dave Rader (R-Tulsa), aimed to tackle this issue by establishing a statewide jail data collection system, but the bill did not make it to the House floor for a vote. Beyond challenges in identifying Medicaid-eligible inmates, a lack of data hampers state leaders' understanding of local jail challenges and their ability to allocate appropriate funding and resources, ultimately undermining the effectiveness of the justice system.
Understanding the reentry waiver
A new Medicaid waiver, announced by the Centers for Medicare and Medicaid Services (CMS) in April 2023, offers a way for states to better support people leaving incarceration during the often-vulnerable reentry period.
The Section 1115 reentry waiver (also called a “demonstration opportunity”) allows Medicaid to pay for a limited package of transitional services for up to 90 days before a person’s release from jail or prison.
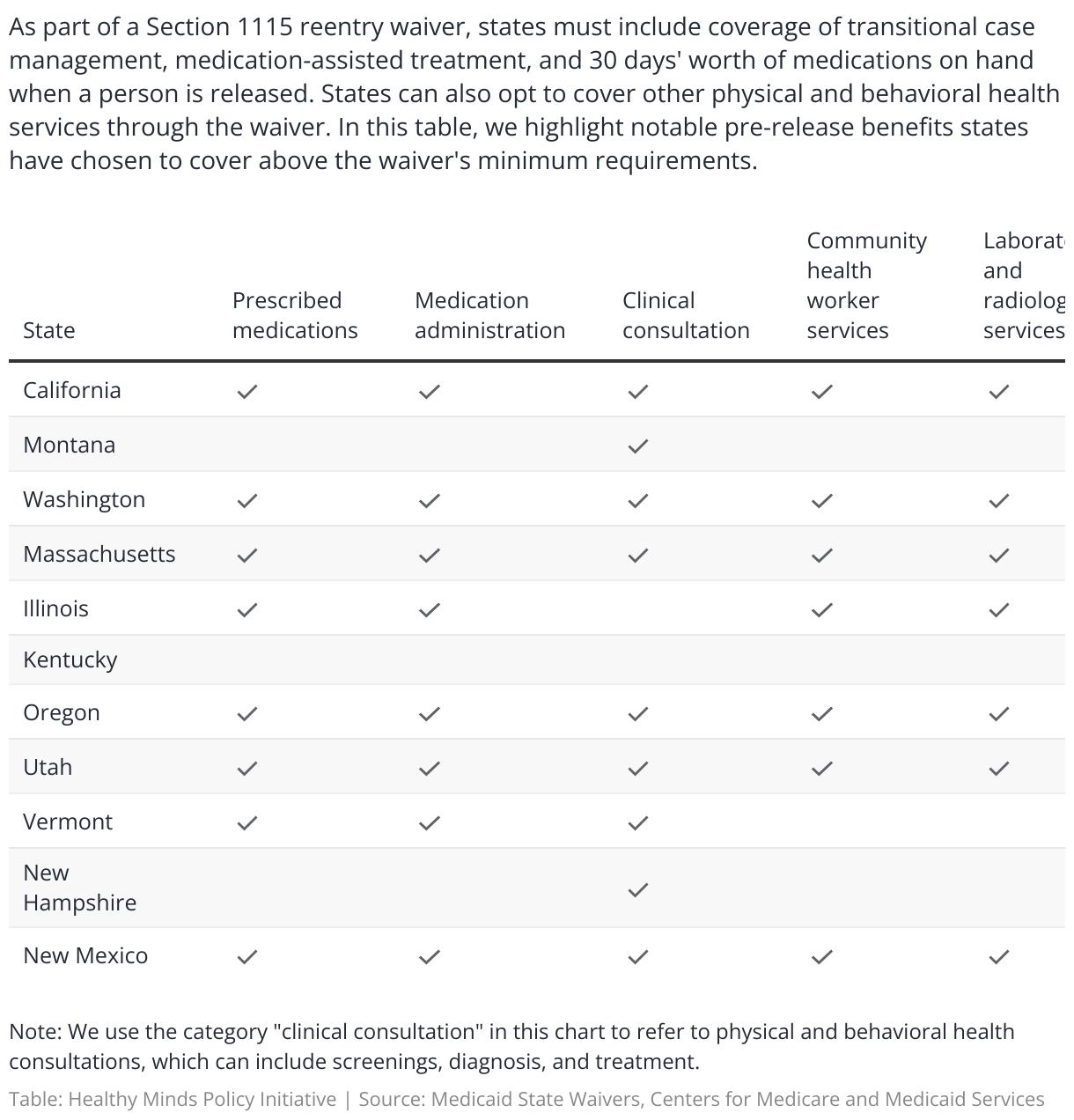
Under the waiver, the benefits package must include coverage of reentry transitional case management, medication-assisted treatment, and 30 days’ worth of medications on hand.
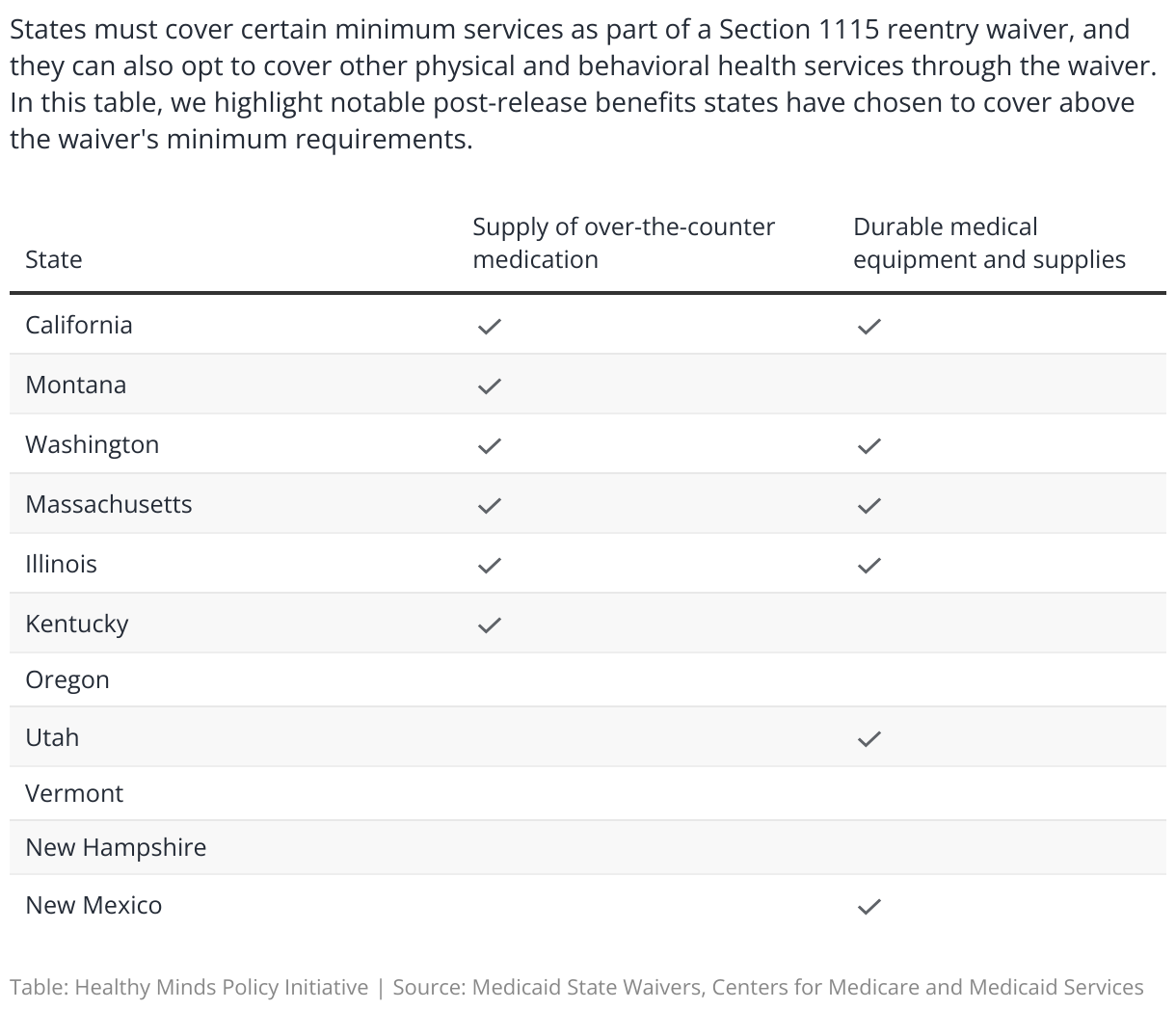
Some states have also received CMS approval to provide other physical and behavioral health services, as well as medications and medication administration, outreach and educational services from community health workers, and medically necessary durable medical equipment (such as wheelchairs, prosthetic devices, or diabetic supplies) to better prepare individuals leaving the justice system for success. This approach can also address underlying issues contributing to an individual's initial incarceration.
Who can be covered under the waiver
States can use the waiver to cover all Medicaid-qualifying incarcerated individuals for up to 90 days before their release. Some states have opted to limit this further, narrowing the population to covering only individuals with chronic medical or behavioral health conditions, and only offering coverage for 30 days before their release.
States also can choose which facilities, such as state prisons, local jails, and youth correctional facilities, will participate in the waiver. They can offer services in all eligible facilities or only in a select few, and they may use a gradual approach, starting with a few facilities and adding more over time. Federal prisons are excluded, but state Medicaid agencies can work with federal prisons to inform individuals about how to apply for Medicaid in the state they will live in after their release.
Benefits and flexibility for states
One of the critical aspects of the Reentry 1115 waiver is the flexibility it offers states in determining the coverage of specific services and medications above the waiver’s requirements. CMS has been clear that it will not allow states to offer coverage of the entire Medicaid benefit package to incarcerated people. Still, there is enough flexibility to allow states to tailor their transitional limited benefit package to best meet the needs of their justice-involved population, including offering services such as family planning, health screenings, and durable medical equipment in addition to required services.
States can also define the pre-release timeframe for providing these services, allowing for a transitional period of 30 to 90 days. This period is crucial in ensuring that individuals have the necessary care and support as they prepare to re-enter the community, ultimately increasing their chances of successful reintegration and reducing the likelihood of recidivism.
Through the waiver, states must reinvest any new federal funds received into initiatives that enhance access to or the quality of health care for incarcerated individuals. This commitment could involve expanding Medicaid services, improving carceral health care, investing in health information technology, or developing other community-based reentry services to meet the health-related social needs of justice-involved populations.
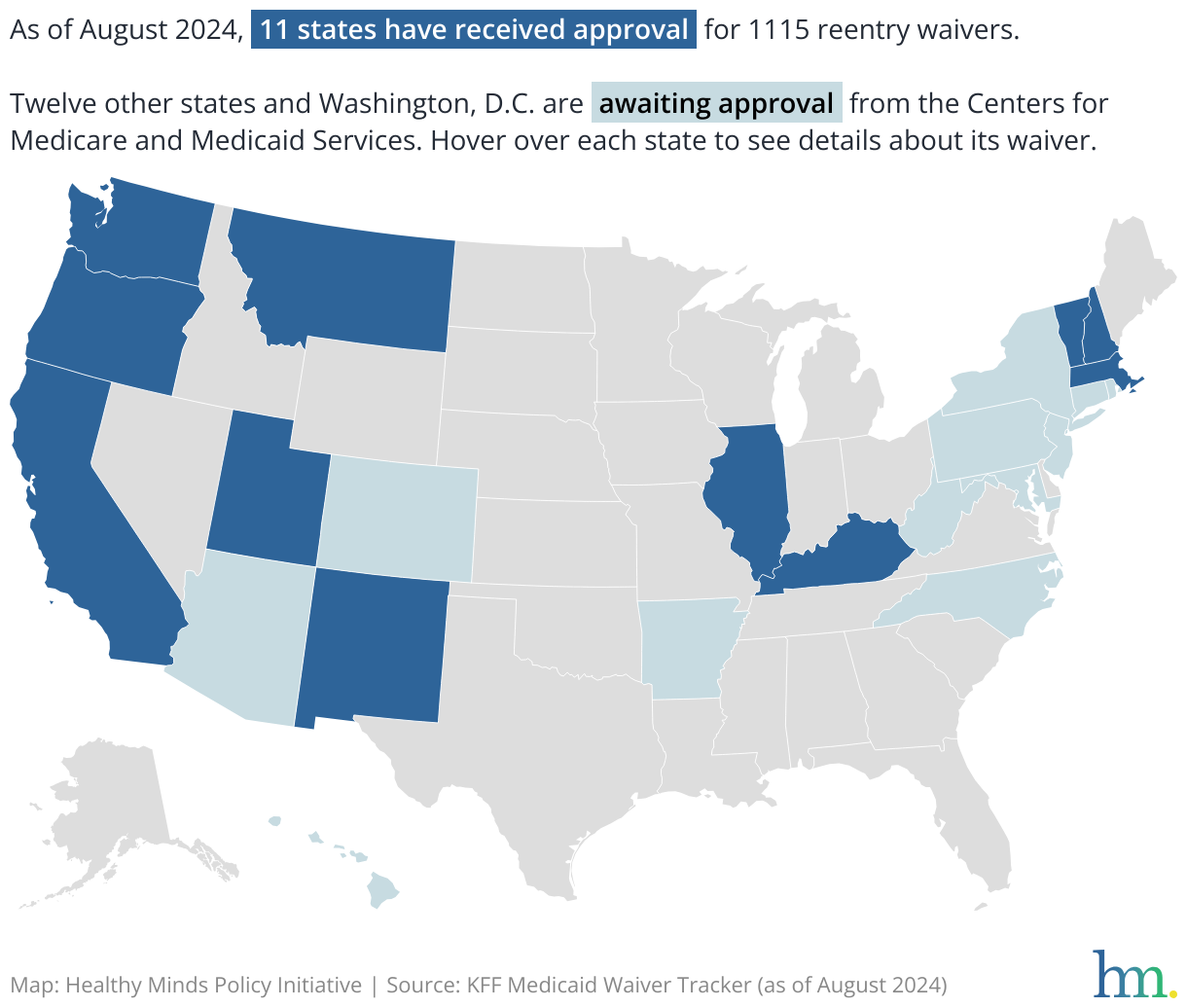
States with approved or pending Medicaid Section 1115 reentry waivers
Waiver financing
CMS requires 1115 waivers to be budget neutral, which means that any new spending under the waiver cannot surpass what would have been spent under the regular Medicaid program.
To ensure a waiver is budget neutral, the federal government first determines the baseline spending by calculating how much would have been spent on Medicaid without a waiver. Then, the state creates a plan for how it will spend money under the waiver by estimating costs based on its new approach. The state must show that its new approach will cost the same or less than the baseline spending. If the waiver results in higher costs, the state is responsible for the additional costs.
States can keep costs lower by defining a waiver’s target population. For example, states can tailor a waiver application to support people with the highest needs, such as people with disabilities, chronic health conditions, substance use disorder, or those with severe mental health needs. Using this kind of targeted approach, a state can ensure resources are allocated where they are most needed, mitigating costs while supporting those most in need.
Using the reentry waiver to meet other federal requirements
Beginning in January 2025, states will have to update Medicaid and Children's Health Insurance Program, or CHIP, plans in accordance with the Consolidated Appropriations Act (CAA) of 2023, which requires states to provide specific services for eligible justice-involved youth.
The Act requires states to provide targeted case management and Early and Periodic Screening, Diagnostic and Treatment (EPSDT) services -- which includes medical, dental, vision, hearing and behavioral health screenings -- to eligible youth for a minimum of 30 days before and 30 days after release from incarceration.
Oklahoma has been working toward meeting the January 2025 implementation timeframe for these new requirements. As part of these changes, states may also choose to extend Medicaid coverage to unsentenced incarcerated youth while they wait for their charges to be resolved.
To streamline these changes and reduce administrative burdens, CMS has advised states to cover these newly required services for justice-involved youth under the Section 1115 reentry waiver, rather than dividing these services between a waiver and an amendment to a Medicaid state plan. A Medicaid state plan is the written agreement between a state and the federal government about how the state will administer its Medicaid program, whereas a waiver allows states to offer additional, optional services or expand eligibility to groups who would not otherwise meet Medicaid requirements.
With the flexibility of the reentry waiver, states can opt to cover more services and a wider swath of incarcerated people for a period longer than 30 days while still meeting requirements for justice-involved youth.
Implications for Oklahoma
Oklahoma can join other states in using Medicaid to provide a smoother and safer reentry period for the thousands of residents released from incarceration every year.
Because Oklahoma has an existing Section 1115 waiver, the state can amend its current waiver to include components of the reentry 1115 waiver. In fact, CMS has encouraged states to combine waivers rather than submitting separate ones to save time and streamline efforts for the state’s Medicaid agency.
With Oklahoma’s high incarceration rates, amending its 1115 waiver to include reentry services would ensure continuity of care and foster crucial community connections for people leaving the criminal justice system, supporting many recommendations for Oklahoma identified by the governor’s MODERN Justice Taskforce.
At the same time, Oklahoma should consider addressing data collection gaps that hinder policymakers’ and agencies’ insight into the potential Medicaid eligibility of the state’s incarcerated population. Establishing a statewide jail data collection system, like Rep. Blancett and Sen. Rader’s HB 3848 would have done, would help the state develop a clearer picture of incarcerated Oklahomans’ circumstances. More robust data collection would work hand-in-hand with a waiver to include reentry services, helping the state identify people who can benefit from support as they transition back into the community after incarceration.
By offering health coverage and transitional services during the critical reentry period, Oklahoma can realize cost savings for the state and better mental health outcomes for formerly incarcerated people.
Appendix: Section 1115 reentry waivers in other states
Eleven states have approved Section 1115 reentry waivers: California, Massachusetts, Montana, New Hampshire, Washington, Illinois, Kentucky, Oregon, Utah, Vermont, and New Mexico. Twelve other states and Washington, D.C. are awaiting approval. Most states with approved waivers offer a 90-day eligibility period for individuals in correctional facilities before their release, except Montana, New Hampshire, and Kentucky, which have eligibility periods of 30, 45, and 60 days, respectively.
Most states provide a wide range of benefits, such as case management, medication-assisted treatment (MAT) with counseling, health consultations, medication, community health worker services, laboratory and radiology services, and a 30-day supply of medications upon release.
Montana and Kentucky offer more limited benefits without clinical consultations and community health worker services. Oregon, Utah, and New Mexico stand out for including family planning, Hepatitis C treatment, and peer support services, which are not uniformly available across other states. Vermont also includes peer support services, treatment for Hepatitis C, and screening for common health conditions as part of its unique offerings. The differences in services underscore how a state balances comprehensive care and limitations when addressing specific health needs within its correctional systems.
Optional pre-release services covered under states' Section 1115 reentry waivers
Optional post-release services covered under states' Section 1115 reentry waivers