
The impact of managed care on Programs of Assertive Community Treatment
Medicaid is the single largest payer for behavioral health services in the United States, with nearly 20% of Medicaid enrollees living with a behavioral health diagnosis. As of January 2023, more than 1.3 million Oklahomans are enrolled in SoonerCare, Oklahoma’s Medicaid program. The Oklahoma Health Care Authority will make significant changes to SoonerCare during the next 12 months as it transitions to a managed care model of payment for services delivered to a significant portion of these Medicaid enrollees.
Most states that adopt a managed care model over the traditional fee-for-service reimbursement system do so to reduce program costs while improving performance, quality, and health care outcomes. However, some states similar to Oklahoma have seen worse mental health outcomes after transitioning to a managed care system. The transition could be felt most acutely by Oklahomans who rely on intensive services to manage their behavioral health conditions.
Among these services is the Program of Assertive Community Treatment (PACT), an evidence-based treatment model for individuals within the community who experience severe mental illness and are high utilizers of other systems, including hospitals and the criminal justice systems. PACT is administered by self-contained, integrated clinical teams that offer a fixed point of responsibility, rehabilitation, and support. The team is available any day, at any time, and provides services to their consumers where they live. This flexibility to meet consumers’ needs is enhanced by additional evidence-based practices such as Supportive Employment and Illness Management and Recovery.
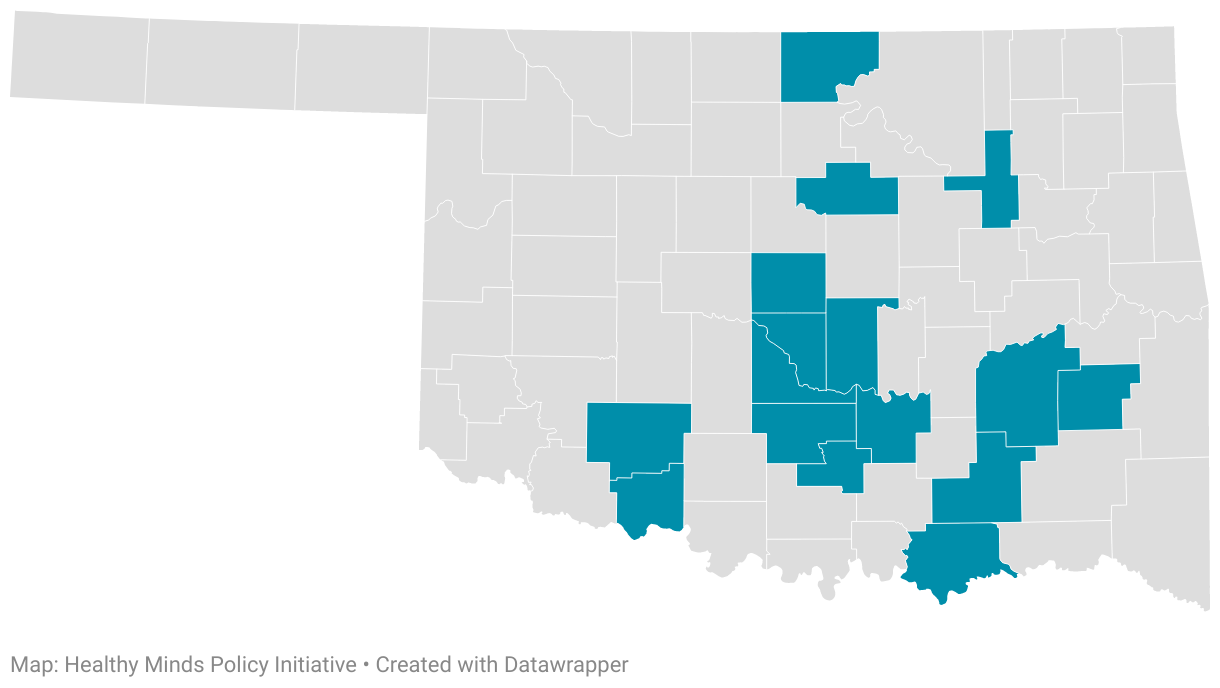
Eight organizations provide PACT services to roughly 800 Oklahomans through contracts with the Oklahoma Department of Mental Health and Substance Abuse Services.
PACT team coverage by county
Taking lessons from other states, Oklahoma providers and regulators can ensure continued positive outcomes from intensive mental health services like PACT during the state's transition to Medicaid managed care.
Background: Managed care in Oklahoma
A Medicaid managed care organization (MCO) is contracted by the state to manage the cost, utilization, and quality of state-purchased health insurance for people who receive health benefits through the state’s Medicaid agency. Through Medicaid MCO contracting, Medicaid agencies pay MCOs a set payment per month, or capitation, for each Medicaid member they serve.
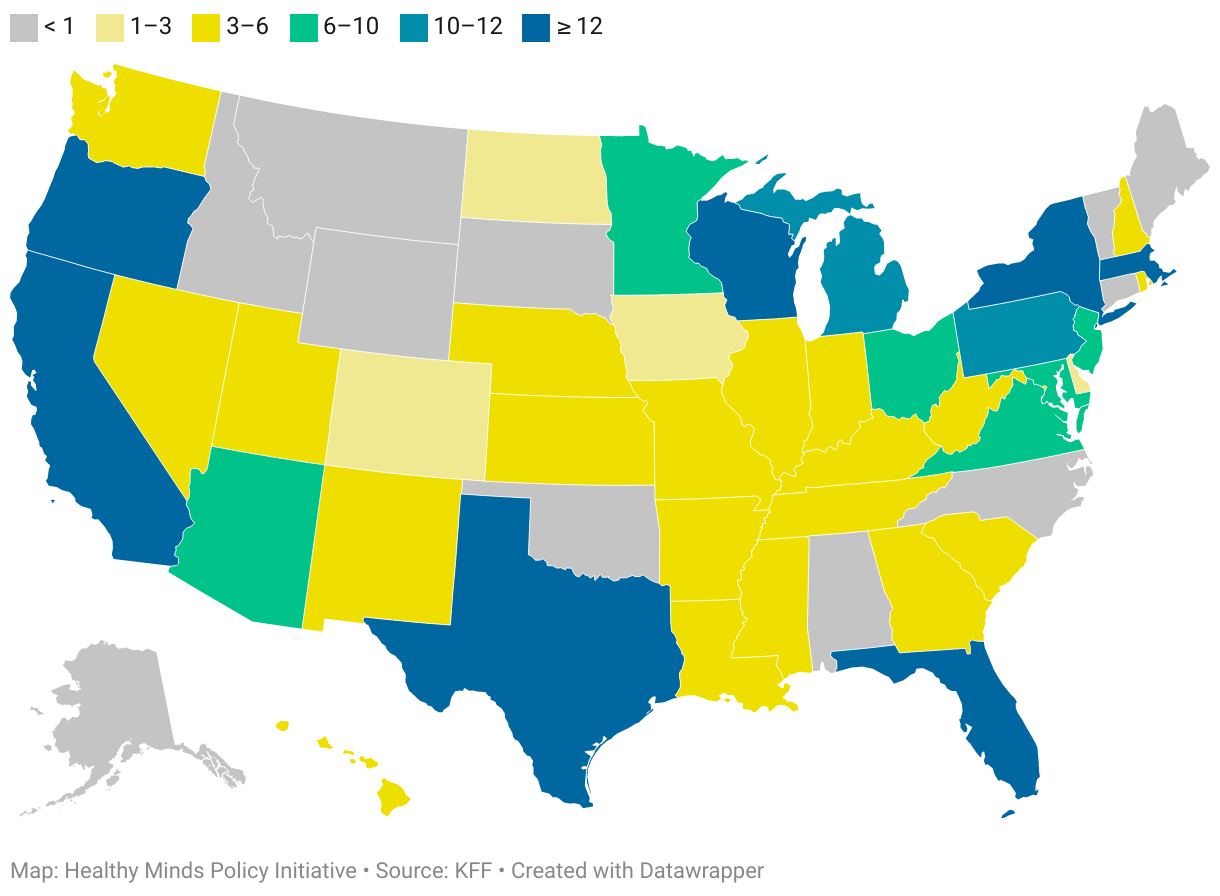
Medicaid managed care organizations by state, 2020
In 2022, Gov. Kevin Stitt signed into law SB 1337, authorizing the Oklahoma Health Care Authority (OHCA) to create a new MCO-run Medicaid program. SoonerSelect, as the program will be known, will contract with three MCOs to manage care initially for specific Medicaid populations: children, pregnant women, deemed newborns, parents and caretaker relatives, and adults aged 19 to 64 with an income at or lower than 138% of the federal poverty level. SoonerSelect is set to take effect on April 1, 2024, contingent on CMS approval.
Many of the Oklahomans served by PACT teams are among populations that will remain in the fee-for-service SoonerCare program. If MCOs show cost savings and improved health outcomes, these individuals could soon fall under the purview of MCOs. Mercer, a consulting firm contracted by Oklahoma to draft the MCO request for proposals, indicated during a presentation to prospective MCOs that these organizations could produce cost savings by cutting behavioral health services through their at-risk managed care adjustment assumptions. This cut in behavioral health services is assumed to be mitigated through consumers’ primary care providers. However, primary care professionals are not yet equipped to handle specialty behavioral health care like PACT and other costly services, which would most likely be impacted by any cut in services.
Lessons from other states
Oklahoma can learn from the dozens of other states that utilize MCOs to deliver Medicaid services. Healthy Minds interviewed behavioral health care providers in Nebraska and Texas to better understand the challenges and opportunities ahead for PACT teams during Oklahoma’s MCO transition.
In Nebraska, de-authorizations from the MCO resulted in many individuals discharging quickly from their PACT teams. MCOs observed stability, but not improvement, in the individual, implying that the individual had reached their baseline and could be discharged from the team. Unfortunately, community mental health providers noted that many of these individuals came back to the PACT team sicker and in some cases were unable to get back to that initial baseline, or at the very least it was much more difficult.
These changes were detrimental to both patients and the PATC team staff. Morale dropped as staff no longer saw the same successes as before patients lost coverage for PACT services. Although individuals should not receive PACT services for life, providers should decide who needs these services, not the MCO pre-authorization process.
Texas recently transitioned all of its Licensed Mental and Behavioral Health Authorities to Certified Community Behavioral Health Centers (CCBHCs). CCBHCs benefit from enhanced federal funding from the Substance Abuse and Mental Health Services Administration and operate under a prospective payment system (PPS), a lump sum for each patient that allows for mix-and-match services better adapted to their needs and treatment plan. This transition to a PPS, in addition to the contracting of MCOs with capitation rates very similar to the PPS rate, has allowed insurers to tie their MCO capitation rates to providers’ PACT outcomes, creating a value-based system of reimbursement.
An organization in Texas noted how the MCOs relied on local mental and behavioral health authorities to authorize PACT services, who in turn would bill the MCO. There has also been a recent shift in Texas requiring MCO contracts to have 50% of their services for capitation be value-based, evaluating the overall outcomes of the team rather than individuals’ outcomes to determine treatment success. By gathering all the outcomes, cost savings, and return on investments, the team helped emphasize the importance of a value-based system, and MCOs continue to invest in the PACT team and their services with a bundled rate. This allows for the flexibility required within the PACT model and recognizes that while PACT is not for life, it can take a longer and less direct course of treatment that an individual-based outcome model cannot always account for.
Recommendations for ensuring high-quality PACT services
Considering the examples above, providers should consider the possible impact a transition to MCOs could have on PACT service delivery. The following recommendations could reduce interruptions in services for an especially high-need population.
Preparing for changes to pre-authorization
It is important to communicate to each PACT team exactly what the MCO requires for authorization and what language/terminology is needed to meet the criteria of medical necessity. MCOs tend to lean toward more medical disease language, which is not always the case for PACT service providers and could lead to unnecessary and harmful delays and de-authorizations. Ensuring that staff members understand and know how to apply this language provides the best chance of continued authorization for their consumers. It is paramount to avoid those instances of increased symptomology and sickness as seen in Nebraska.
Encouraging team value-based billing
Using a value-based approach for metrics, as Texas does, will allow PACT teams to continue serving individuals who are both stabilized and in later stages of change without prematurely discharging them – this is a way of looking at how an individual integrates new behaviors, goals, or programs. To prevent the negative outcomes seen in Nebraska, value-based metrics recognize that PACT serves individuals in different ways. If the team shows transitions to lower levels of care and system savings overall, the MCO’s decision to cover PACT services should not be based on the individual who is already eligible for the program. Aligning MCO contracts with evidence-based best practices and PACT eligibility criteria would continue to allow PACT teams the autonomy they need to achieve their desired outcomes.
