
How Oklahoma can reduce housing insecurity through Medicaid
Access to safe, stable, and affordable housing is foundational for a person’s overall health and well-being. But securing housing is a challenge for many in Oklahoma: between 2022 and 2023, the number of Oklahomans experiencing homelessness increased from 3,754 to 4,693, a 25% rise in a year.
Housing insecurity and behavioral health needs are intertwined: when people lack secure housing, they also often face difficulties in accessing health care services, leaving their physical and mental health needs unmet. In 2023, 23% of individuals experiencing homelessness in Oklahoma — including people living unsheltered, in transitional housing, or in an emergency shelter — had a severe mental illness, and 21% had a chronic substance use disorder.
As states look for strategies to address the complex challenges of homelessness, Medicaid can be part of the solution. While Medicaid alone cannot solve a shortage of affordable housing, it can make a significant impact by providing health care and support services to members experiencing homelessness or housing insecurity.
In this analysis, we explore how Oklahoma and other states can utilize strategies through Medicaid to address housing insecurity for Medicaid members with serious mental illness or substance use disorders.
Key takeaways
- Supportive housing programs can improve health outcomes, reduce emergency department visits, and lower health care spending. Funding housing-related supports through Medicaid is likely to produce similar results.
- Demonstrating a growing interest in funding whole-person health care, the federal Medicaid agency has encouraged states to address health-related social needs through Medicaid, including providing housing support.
- Oklahoma can explore several Medicaid strategies — including state plan amendments, health services initiatives, and waivers — alongside community partnerships with behavioral health clinics and housing agencies to address housing insecurity for SoonerCare members.
Background
In Oklahoma, more than 1 million low-income residents have health coverage through SoonerCare, the state’s Medicaid program, which is managed by the Oklahoma Health Care Authority. While Medicaid has traditionally focused on providing coverage for medical services — like office visits, hospital stays, and prescription drugs — there is growing interest in and awareness of using Medicaid to address enrollees' health-related social needs, or HRSNs.
Health-related social needs are the economic and social conditions that affect people’s health and well-being. This term is similar to “social determinants of health,” and the two can sometimes be used interchangeably.
For this analysis, social determinants of health refer to the broader, population-level conditions that affect the way people live. In contrast, health-related social needs are the individual, immediate social and economic conditions a person must have to maintain their well-being. So, while access to housing can be shaped by systemic discrimination and poverty — which are social determinants of health — a person’s individual need for safe and stable housing is a health-related social need.
Medicaid programs around the country, with support from the Centers for Medicare and Medicaid Services (CMS), are experimenting with funding services that address health-related social needs to improve health outcomes and reduce health care costs, including housing support services.
CMS first issued guidance to states on addressing health-related social needs through Medicaid in 2021. Since these are relatively new strategies, there has been limited research on the effectiveness of Medicaid programs in addressing health-related social needs. However, research has shown that access to healthy food, safe housing, transportation, and other health-related social needs can significantly improve health outcomes and reduce government spending. Studies have also shown that supportive housing programs can improve health outcomes, reduce emergency department visits, and, as a result, lower health care spending.
As more states use Medicaid to offer these kinds of services, we expect outcomes data will become more readily available.
Strategies for addressing housing insecurity through Medicaid
States have several options for implementing housing-related supports through Medicaid.
Each state Medicaid program operates under a state Medicaid plan, a written document that outlines how the program will function. It details what services Medicaid covers, how providers are reimbursed, and information about enrollment and eligibility.
States can add to or change their Medicaid plan through a state plan amendment, a written request that goes to CMS for approval.
In this section, we outline four pathways states can take to offer housing-related supports through Medicaid, including state plan authorities, Children's Health Insurance Plan (CHIP) health services initiatives, managed care arrangements, and waivers. Each of these strategies requires approval from CMS.
State plan authorities
States can incorporate optional Medicaid benefits to address health-related social needs under Section 1905(a) of the state plan authority. These benefits can include rehabilitative services (such as peer support services) and targeted case management, which can help individuals coordinate health care and social supports, like housing, transportation, employment, and nutrition services.
For example, Louisiana Medicaid modified its state plan to include permanent supportive housing agencies as peer support service providers, who can review members’ referrals and check their eligibility for the permanent supportive housing program.
Home and community-based service options
States can also choose to offer housing support services through a home and community-based services waiver or state plan amendment.
State plan amendment option
Through a Medicaid home and community-based services state plan amendment, states can offer a variety of services targeted to specific populations, such as people with developmental disabilities, physical disabilities, mental illness, or substance use disorders.
Texas has implemented such a program through a state plan home and community-based services benefit, called Home and Community-Based Services for Adult Mental Health, which offers services aimed at supporting long-term recovery from mental conditions. The program provides housing-related assistance, such as helping individuals resolve conflicts with landlords or neighbors, connecting them with community resources to prevent eviction, reviewing and updating their recovery plan (which includes housing support plans), and identifying services that can help with moving costs and one-time expenses.
Waiver option
A Medicaid home and community-based services waiver allows states to offer long-term services and supports in home and community-based settings to those who would otherwise need institutional care. With CMS approval, states can waive standard federal requirements and provide services that would normally be outside of typical Medicaid coverage.
Recently, states have used this type of waiver to cover services that focus on health-related social needs to help individuals achieve community integration goals while maximizing their independence and safety in their homes. One of these services is housing and tenancy support, which involves assessing an individual's community integration needs, assisting in finding and securing housing and helping with completing housing applications.
For example, Louisiana's Adult Day Health Care waiver covers one-time costs for transition services (such as utility deposits and essential furnishings) for people moving from nursing facilities to private residences. Similarly, Louisiana’s Community Choices waiver provides housing stabilization services to help participants maintain tenancy in the state’s Permanent Supportive Housing units.
Children's Health Insurance Plan (CHIP) Health Services Initiatives
Another avenue for states to offer housing-related supports is by presenting a proposal to CMS for Health Services Initiatives (HSIs) that improve children’s health through Medicaid. These initiatives can address health-related social needs through direct services, public health programs, and social or behavioral health needs.
Recently, using this strategy, Wisconsin became the first state to receive federal approval to provide housing benefits to low-income families in need. Families with children aged 18 or younger and pregnant individuals with low income (below 200% of the federal poverty level) and without housing are eligible for this benefit through one of the eight homeless assistance providers selected for this initiative. The approved housing support services include housing consultations, transition support, relocation support of up to $2,000 per relocation event, and ongoing support.
HSIs receive funding from state and federal sources, with the state drawing federal funds from its CHIP administrative allocation. These funds are provided at the state's CHIP match rate and are subject to a 10% cap. Oklahoma would be in a position to submit a similar initiative providing housing support to children and families, since it has yet to reach its 10% cap.
Managed care organizations
States can also use managed care contracts to address housing instability for people with severe mental illness. One way to achieve this is by incentivizing — or requiring — Medicaid managed care organizations (MCOs) to screen and coordinate care for members' health and social needs. MCOs are private insurance companies contracted by a state Medicaid agency to deliver Medicaid services.
Under Oklahoma’s Medicaid managed care program, SoonerSelect, MCOs will screen enrollees to determine their health-related social needs and refer enrollees to appropriate social services organizations. In addition to tracking the outcomes of those referrals, MCOs will also work with community-based organizations or social service providers to ensure enrollees receive the necessary support.
Some states have gone beyond the usual requirements in their MCO contracts by including specific provisions requiring certain screening tools or referral systems. For example, North Carolina mandates using NCCARE360, a statewide network that brings together health care and human services organizations. This technology lets providers electronically connect individuals who need assistance with relevant community resources, while also ensuring feedback and follow-up for effective service delivery. Some states require specific health-related social needs questions in the screening tool, while others require using a tool that the state has approved.
Additionally, states can encourage MCOs to offer value-added services that cover housing-related supports. Value-added services are extra services provided by managed care plans to improve care and reduce costs, funded through the plan’s administrative funding.
Though there was a slight decrease between 2022 and 2023, most managed care health plans offer HRSN services for unhoused or housing-insecure individuals, indicating that these organizations recognize the importance of addressing housing insecurity as a determinant of health. In 2023, 83% of MCOs offered HRSN services, down from 90% the previous year, according to an annual Medicaid MCO survey.
Soon, managed care organizations in Oklahoma will begin offering value-added services to more than 800,000 SoonerSelect members. Examples of their housing-related offerings include:
- A rewards program that incentivizes members to adopt healthy behaviors. Members will receive a pre-loaded Visa card, which they can use to pay for groceries, utilities, cell service, non-covered transportation, gas expenses, retail stores, housing and rent support, and educational needs.
- Housing assistance to members of up to $350 per year to help with housing expenses like apartment rent or mortgage payment, internet and utility bills, and moving expenses.
- Transitional housing to members discharged from an inpatient treatment facility for substance use. Those who qualify may be eligible for funding for short-term housing up to $1,200 monthly for three months.
These types of service offerings are important steps in addressing housing insecurity in Oklahoma. However, the state could take further steps by working with MCOs to ensure housing specialists are on staff. At least one of Oklahoma’s MCOs has housing specialists on staff, and another offers housing-related services through care coordinators. Oklahoma could ensure consistency across MCOs by developing staffing requirements for housing specialists. Several states, including Louisiana, Arizona, and New Jersey, have implemented housing specialist positions within MCOs. Housing specialists support case managers by providing education and training on evidence-based housing interventions, identifying and referring members with housing needs to appropriate services, and tracking referrals.
Oklahoma could also require MCOs to collaborate with a local housing agency, as Louisiana has done. These types of collaborations can help identify members in need of services, authorize housing support services, and contract with housing providers. By partnering with local housing agencies and hiring dedicated housing specialists, MCOs can extend their reach and ensure members can access resources to address housing insecurity.
Section 1115 demonstrations
CMS requires states to exhaust other previously mentioned Medicaid strategies before applying for a Section 1115 waiver. Since Oklahoma has not utilized all the Medicaid authorities available to tackle housing instability, applying for an 1115 waiver would not be the initial step to begin providing housing support services through Medicaid.
An 1115 waiver allows states to deviate from specific federal Medicaid program requirements and test new health care delivery models and approaches focusing on improving health outcomes and reducing costs. It is a practical approach that enables states to have the flexibility to establish partnerships with community-based organizations and offer services that Medicaid does not typically cover, including services that address non-clinical services, such as housing, food, and transportation.
Additionally, waivers allow states to target eligibility for HRSN services to high-need populations, add services to the benefits package, and require health plans to provide them to eligible enrollees. Furthermore, it covers a broader range of Medicaid beneficiaries with clinical and social risk factors than the 1915(c) waivers, which are more specific to elderly or disabled individuals.
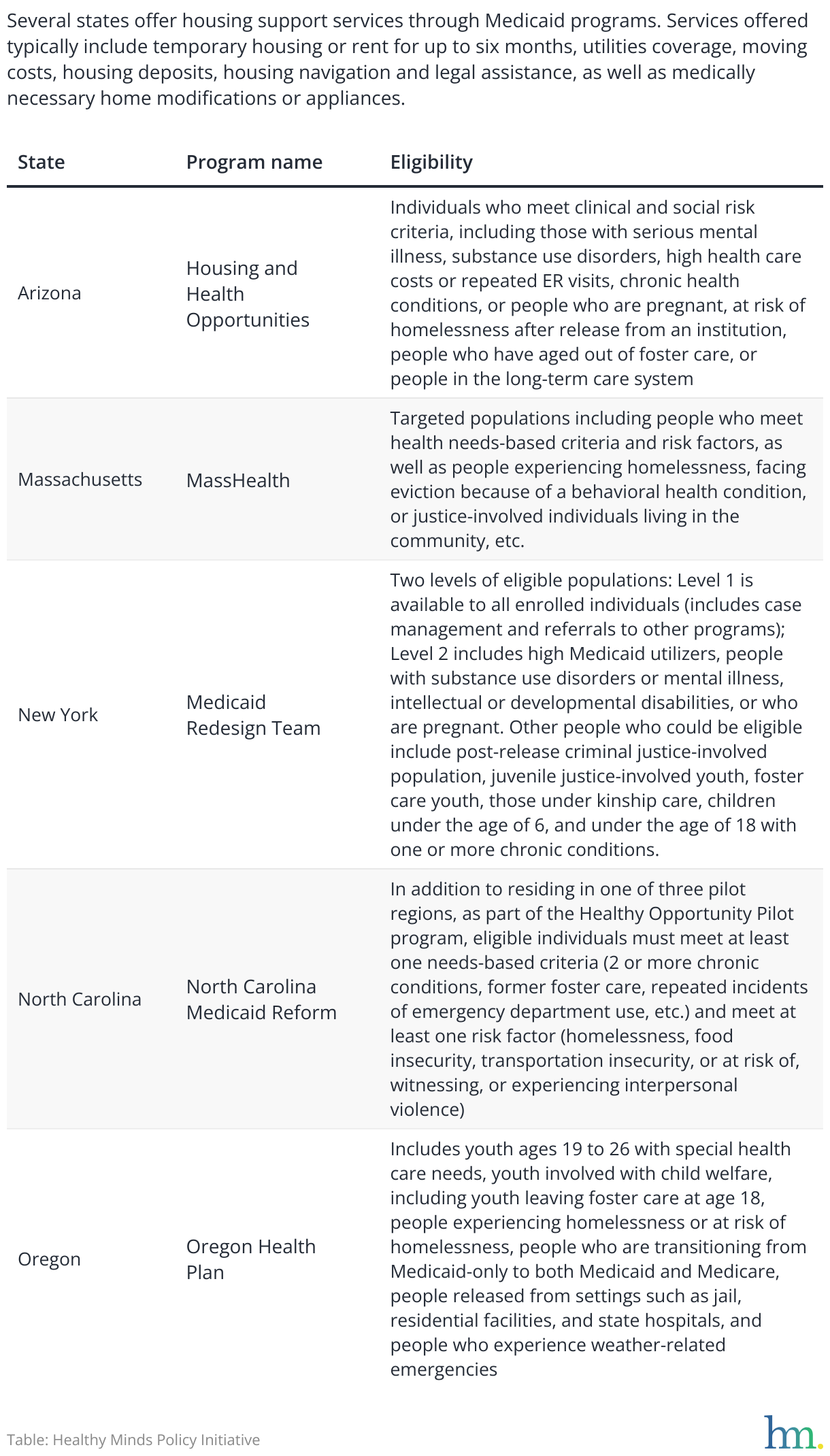
CMS has approved 1115 waivers for housing supports in 18 states, and the agency has recommended other states follow the examples of waivers in Oregon, Massachusetts, and New York because of how these states’ waivers prioritize whole-person care. Other examples of states with successful 1115 waivers are Arizona and North Carolina.
When Oklahoma has exhausted other Medicaid options for addressing housing instability among its members, the state could look to any of these states’ examples of implementing innovative models to tackle the housing needs of specific Medicaid populations.
The waiver approvals indicate a shift towards a whole-person care approach that recognizes the role of social barriers in worsening health outcomes and driving health care spending.
Table: State Medicaid 1115 waivers to fund housing supports
To support the infrastructure around states’ programs to address health-related social needs, CMS has also granted states funding that can be used, for example, for developing electronic referral systems, creating policies for referral management, providing cultural competency and trauma-informed training to staff, and designing outreach and education materials.
Implications for Oklahoma
Oklahoma can take a holistic approach to addressing housing insecurity and other health-related social needs using both the strategies we have outlined through Medicaid as well as partnerships with community-based organizations.
Partnerships between Medicaid agencies and Certified Community Behavioral Health Clinics or local housing agencies, for example, can ensure members connect with housing-related resources that promote their overall health and well-being. Housing support can allow individuals with mental health or substance use disorders to better access and engage in treatment, leading to improved outcomes.
Oklahoma has many opportunities to address homelessness and housing insecurity through Medicaid, and state agencies must explore and leverage the tools they have to meet residents’ unmet health and social needs. Solving this complex issue will require a comprehensive approach that addresses the root causes of homelessness and housing insecurity, and how these issues are intertwined with behavioral health needs.
