
How Oklahoma can prevent unnecessary Medicaid coverage losses under H.R. 1
In 2027, Oklahoma’s Medicaid program will impose new work requirements and more frequent eligibility checks because of H.R. 1, the 2025 federal budget bill that made sweeping changes to how states fund and administer their Medicaid programs.
These changes will affect thousands of Oklahomans, including many who access behavioral health services through Medicaid. Nationally, Medicaid covers nearly one-third of adults with mental health conditions and one-fifth of adults with substance use disorders.
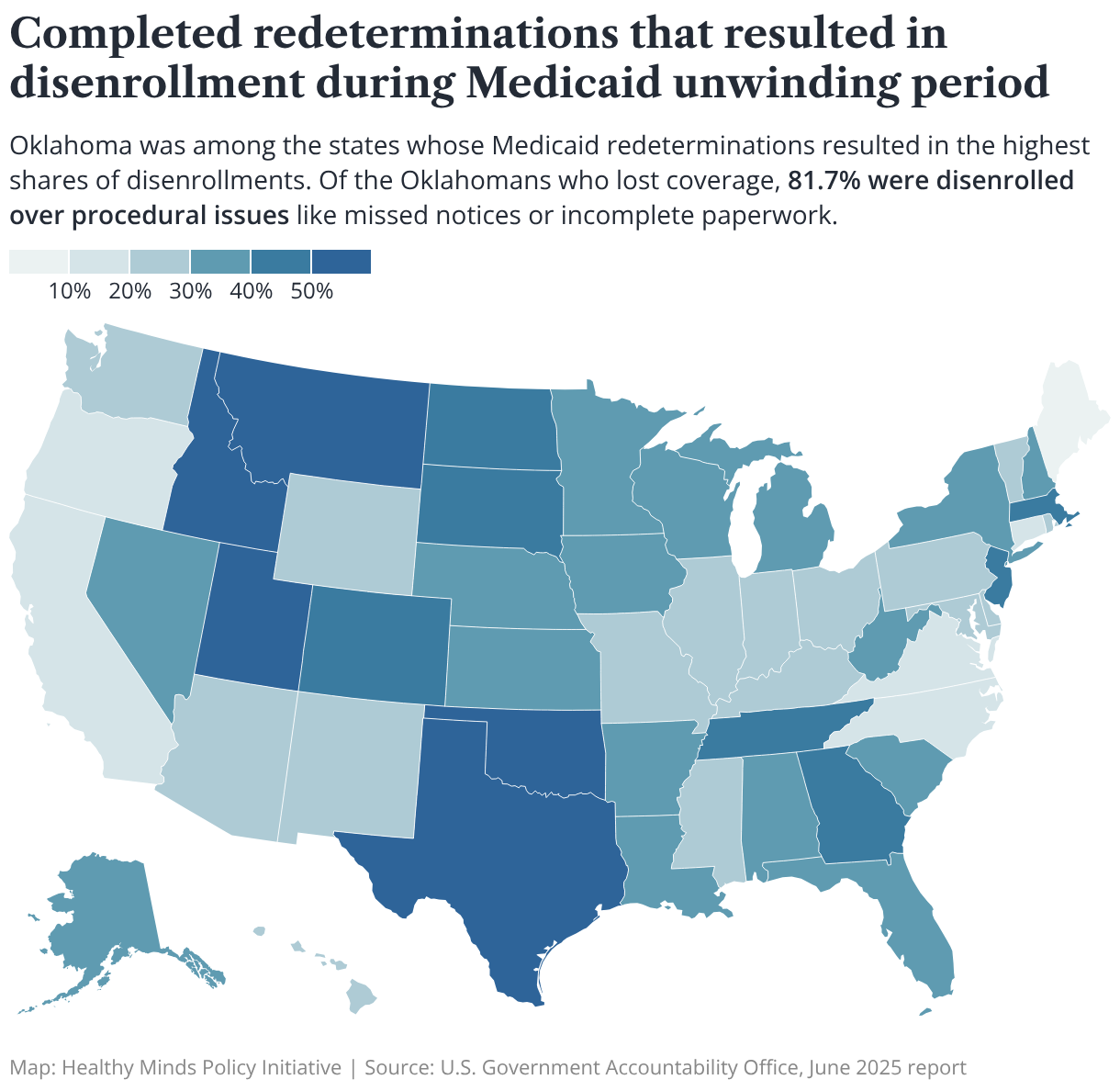
As Oklahoma recently saw during the “unwinding” of continuous Medicaid coverage during the COVID-19 pandemic, potential coverage losses under H.R. 1 are likely to stem from administrative hurdles, more so than ineligibility.
Of the roughly 766,000 Oklahomans who lost Medicaid coverage during the unwinding, about 82% were disenrolled because of procedural issues like missed renewal notices or incomplete forms — one of the highest rates in the nation. Nearly a quarter of people who were disenrolled from Medicaid during the unwinding stayed uninsured following loss of coverage.
Even short gaps in coverage can have major health and financial consequences, especially for people with behavioral health conditions: when people lose access to care, their conditions can get worse and force them into more expensive treatment settings, like emergency rooms. One report found that a lapse in coverage for someone experiencing major depression led to a $650 per month increase in care expenses.
In this analysis, we highlight how Oklahoma can use lessons learned from the unwinding to prepare for changes under H.R. 1 and prevent unnecessary losses of health coverage for Oklahomans.
Key takeaways:
- Because we expect most coverage losses under H.R. 1 will stem from administrative issues rather than ineligibility, Oklahoma should take steps to automate eligibility checks using existing, verified data to reduce administrative burdens on enrollees and prevent unnecessary coverage losses.
- In the absence of federal guidance, Oklahoma must clarify who qualifies as “medically frail” for the purposes of exemptions to work or community engagement requirements, including temporary exemptions. Adopting a broad interpretation — one that includes people with mental health conditions who may lack a formal diagnosis — could protect Oklahomans who are at especially high risk for losing coverage.
- New cost-sharing requirements could mean higher copays for Oklahomans on Medicaid, which in turn could mean people delaying or going without needed health care.
Background: 2023 Medicaid “unwinding”
For about three years during the COVID-19 pandemic, states were required to provide continuous Medicaid coverage during the federal public health emergency. States could not disenroll people from Medicaid even if they no longer met eligibility requirements.
When the public health emergency ended in May 2023, states resumed eligibility checks, and people who no longer met eligibility requirements — or who didn't complete paperwork to prove their eligibility — lost their Medicaid coverage. Officials called this process “unwinding.”
Beginning in 2027 under H.R. 1, Medicaid enrollees will have to complete at least 80 hours per month of work, volunteer service, study, or a combination of these activities, to be eligible for coverage.
Related: How federal changes to Medicaid will affect mental health services in Oklahoma
The Oklahoma Health Care Authority (OHCA) estimated that these requirements will affect roughly 126,000 working-age Oklahomans.
Additionally, under H.R. 1, states will have to check eligibility for people in the Medicaid expansion population (low-income adults ages 19 to 64) every six months instead of once a year.
National projections show that as a result of new community engagement requirements and other provisions in the law, H.R.1 could result in 7 million people losing Medicaid coverage, with most losses expected to stem from the procedural issues rather than ineligibility.
Currently, Oklahoma ranks third in the nation for uninsured residents, meaning more coverage losses will risk widening the gaps for access to care. As more people lose coverage, providers could face increases in uncompensated care for people without insurance, threatening the stability of safety-net behavioral health services.
As these new requirements are likely to create additional administrative burden on the state SoonerCare system and on enrollees, Oklahoma can learn from its challenges and strengths during the unwinding to prevent unnecessary coverage losses in the future.
Recommendations to prevent coverage loss and protect access to care
During the Medicaid unwinding, OHCA deployed a phased approach to support Medicaid members and supporting agencies with resources to navigate the changes and avoid coverage losses. The agency can build on the strategies that worked during the unwinding and look to other states that have seen success with other methods, like automated eligibility verification, to address upcoming changes under H.R. 1.
Automate verification processes to minimize administrative burden
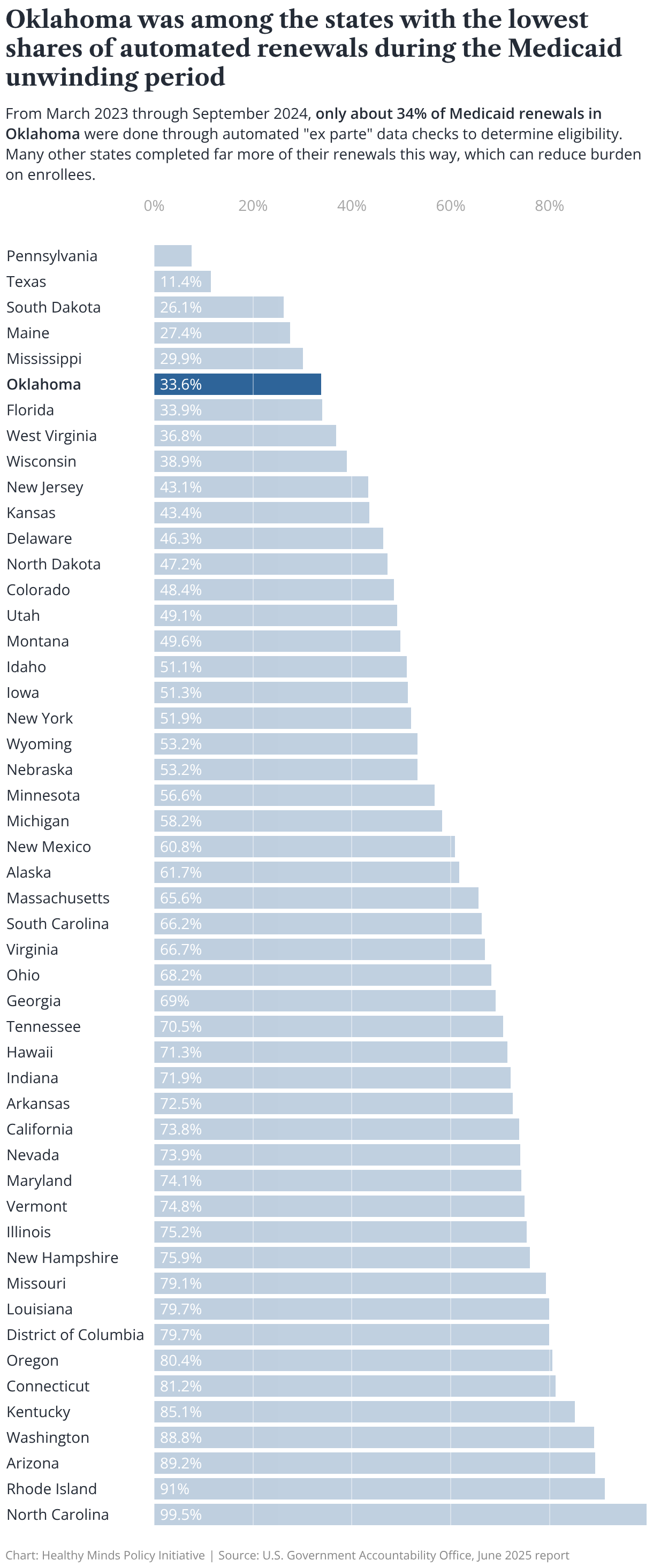
As the state prepares to handle more frequent eligibility checks and implement work requirements, Oklahoma should improve automation of Medicaid eligibility and verification processes to ease administrative burdens on both members and the state SoonerCare system.
When states use automated systems for eligibility verification, they can draw on existing, verified data — like tax records, safety net benefits, or public university enrollment records, for example — to check Medicaid eligibility without the enrollee having to fill out paperwork or respond to a renewal notice.
Another recent study showed that automated systems improved renewal rates by 7.7% and decreased the likelihood of procedural disenrollments by 8.3% in four states. Similar research found that automated renewals are linked to reduced “churning” — coverage disruptions or losses — which suggests that an automated system may provide stability in coverage.
Still, experience from Medicaid unwinding shows these systems must be designed to account for data gaps and errors and must include human review.
For example, if an enrollee’s wage data points to ineligibility but is inconsistent with more recent administrative records or self-reports, an automated system should pause and trigger a review by a state representative. Ensuring human oversight and providing a window for corrections before any final determination would ensure members aren’t erroneously disenrolled because of an automation or data error.
Automated systems should rely on verified data collected through existing federal and state tax records, employment and wage data, Social Security, state's retiree and education systems, public university enrollment systems, safety net benefits enrollment, asset verification, vital statistics, property records, DMV records, and other available administrative data sources to determine compliance or exemptions.
Process automation can be especially helpful for people with disabilities and mental health conditions, as paperwork and reporting requirements can become difficult to manage. Expanding effective automated systems, along with pre-filled and accessible forms, can help reduce unnecessary obstacles to coverage.
In addition to using automated systems to check eligibility, states can use these systems (with approval from the Centers for Medicare and Medicaid Services, or CMS) to proactively extend hardship exemptions for Medicaid enrollees. Hardship exemptions temporarily protect Medicaid enrollees from losing coverage when they cannot meet eligibility requirements for a variety of reasons, including behavioral health conditions, disabilities, or local emergencies.
States should proactively identify members who could qualify for hardship exemptions because of county emergencies or high unemployment rates. And automated systems should regularly screen for changes in circumstances — like a disability or substance use disorder.
Finally, when data to prove an enrollee meets work requirements is unavailable or incomplete, OHCA should allow members to self-report qualifying activities (like volunteering or studying). The agency can cross-check self-reporting with verifiable data and request additional documentation in case of discrepancies.
Adopt broad definitions to prevent vulnerable groups from losing coverage
People who are deemed “medically frail” will be exempt from new work and community engagement requirements under H.R. 1. The law provides five categories that count as "medically frail" — individuals who are blind or physically disabled, have a substance use disorder, have a disabling mental disorder, are developmentally disabled, or have a serious medical condition. But it’s unclear whether guidance from CMS will provide a more detailed definition for each of these categories.
In the absence of a more granular definition or federal guidance, states will have to choose how to interpret this exemption. Mental health advocates and CMS guidance recommend that states adopt the broadest interpretation for “medically frail” to protect vulnerable people from being inappropriately disenrolled or denied coverage.
Advocates suggest aligning the definition of a substance use disorder with standard criteria for a diagnosis, like the Diagnostic and Statistical Manual and International Classification of Disease. Advocates also say exemptions should not be limited based on the severity of the condition or the type of substance.
People with undiagnosed or unreported mental health conditions may struggle to meet work or community engagement requirements, but without documentation, they may not qualify for exemptions if states adopt a narrow interpretation.
Expanding the interpretation for "medically frail" to include people recently released from jail or prison could also prevent loss of Medicaid coverage. Currently or recently incarcerated people are vulnerable to disenrollment or denial of coverage due to work requirements immediately following their release.
H.R. 1 includes a three-month work requirement exemption for people currently or formerly incarcerated following their release. But disabilities, substance use disorders, and complex medical conditions often go undiagnosed or undocumented during incarceration, which could pose challenges for meeting work requirements after the initial post-release period.
OHCA, ODMHSAS, and Oklahoma correctional facilities should work together to develop policies and processes that proactively identify behavioral health conditions during incarceration and provide a longer-term exemption than the three-month post-release period.
In addition to a broad definition for “medically frail,” Oklahoma should adopt a broad “lookback period” for work requirement compliance. A lookback period is a set amount of time during which enrollees must prove they either have met work requirements or qualify for an exemption.
Federal regulation requires up to three months of work compliance history for new enrollees and at every six-month renewal. Oklahoma should seek CMS guidance to determine whether rulemaking would allow a more accommodating lookback period for new applicants. A more flexible lookback period could allow enrollees to use any month within a three-month period prior to their application to meet eligibility requirements.
Within current parameters, if a state chose the last month preceding the application, it could bar an applicant who was working but then experienced a mental health crisis requiring hospitalization from meeting work requirements for the last month.
An adaptable lookback period would allow them to use any month within the three-month window to meet the requirement.
For example, if someone meets work requirements for two months then experiences a mental health crisis and is hospitalized for several weeks, preventing them from meeting work requirements for the next month, they would be allowed to use any month within the three-month window to meet the requirement. This would ensure continued access to care during a period of greater mental health need.
But often, people with mental health needs don’t have a formal diagnosis or records to present as proof. In addition to a three-month lookback period, OHCA should create an option for self-attestation of a mental health condition that might qualify them for an exemption.
Once identified, these individuals should be connected with community mental health programs or services to help them start care, stay engaged with care, and improve their ability to meet work reporting requirements after their needs have been addressed.
Strengthen communication and outreach ahead of changes
Clear and frequent communication will be critical to ensure Oklahomans are aware of the new Medicaid requirements ahead of changes in 2027.
To communicate changes under H.R. 1, OHCA can build on its strong foundation during Medicaid unwinding, when the agency deployed a multi-channel outreach campaign emphasizing renewals and contact updates, as well as a stakeholder toolkit, and community partner engagement.
Federal policy guidance requires that states notify members about upcoming Medicaid changes through traditional messaging such as direct mail, phone calls, and text messages with links to online member portals.
Traditional channels have proven to be effective strategies, with evidence in Maine suggesting phone calls to members assisted over 1,200 households maintain health coverage in a single month. Evidence also suggests that nontraditional targeted messaging including television, radio, video streaming services, public transportation, and billboards can lead to higher renewal retention.
Pennsylvania, for example, used targeted advertisements on nontraditional platforms to reach more people statewide, including television, radio, video streaming services, public transportation, and billboards. Compared to Oklahoma, Pennsylvania saw higher renewal retention, which may be a result of an innovative outreach campaign.
To effectively inform and prepare members, outreach campaigns should align with the application and renewal due dates. Although CMS guidance suggests that outreach be conducted at least once every six months, OHCA should offer ample time to reach members by messaging at least 90 days in advance of the twice-a-year deadlines with accessible and multilingual materials.
The agency could use automated systems for communication around deadlines as well as eligibility issues. Ensuring "SoonerGuide", OHCA's new AI chatbot, is regularly updated on Medicaid program changes to better assist members.
Community partners can serve as a bridge for members to ensure understanding of the new requirements, deadlines, and exemptions, such with Unite Oklahoma and the development of a Partner Resources toolkit during the Medicaid unwinding. Leveraging trusted community organizations could allow for on-site, one-on-one support with document collection and submission, especially for those with language or digital barriers.
Finally, outreach should prioritize people at high risk of disenrollment over procedural issues, including people with mental health needs.
Setting affordable copays for health services
New cost-sharing requirements for the Medicaid expansion population (low-income adults ages 19 to 64) are among the changes coming to Medicaid under H.R. 1.
Previously, states could choose whether to implement cost-sharing for people in the expansion population. Now, co-pays will be required for people in the expansion population, though there are exceptions, including people who are institutionalized and those who receive primary care, emergency care, mental health, substance use treatment, and visits to community health centers, behavioral health clinics, and rural health clinics.
For all other services, the state will set a co-payment up to $35, but it can't exceed the federal limit of 5% of the family's annual out-of-pocket costs. Providers may deny service if a co-pay is not paid but can reduce or waive co-pays on a case-by-case basis.
Currently, Oklahoma imposes lower copays for expansion adults ($4 for most services, $3 for behavioral health and substance use, and $10 per day for behavioral health inpatient care, capped at $75). With the new exemptions, behavioral health and substance use co-pays will likely be removed, which could increase the financial burden on the state.
However, raising the co-pay to the max of $35 per outpatient, specialty services, and prescriptions would significantly impact expansion adults, especially those with chronic conditions. According to a recent KFF analysis, for an expansion enrollee making 100% of the federal poverty level —$15,650 a year — a limit of 5% on out-of-pocket costs would translate to no more than $783/year. However, the analysis found that if the enrollee had three or more chronic conditions, they could pay up to 8% out-of-pocket costs, or over $1200.
Because of these possible barriers, lawmakers should set Medicaid copays at levels that do not create financial barriers or deter eligible individuals from seeking needed care. Establishing higher copays — such as the proposed $35 maximum — risks preventing people from seeking necessary care and increasing costs overall in the long run.
Studies have found that even small cost-sharing amounts lead to fewer visits to medically necessary care, poorer health outcomes, and higher utilization of emergency departments, especially for those with chronic conditions, mental health or substance use needs, and those in need of life-saving medications.
What’s next for Oklahoma
Oklahoma’s experience with Medicaid unwinding revealed valuable lessons the state should apply as it prepares to implement changes under H.R. 1 in 2027.
The stakes for Oklahomans are high: during the unwinding, 82% of Oklahomans who lost coverage did so due to procedural issues, and more than 176,000 Oklahomans stayed uninsured following loss of coverage.
The risk of coverage loss or denial over H.R. 1’s new work requirements is also high, especially for people with undiagnosed mental health and substance use disorders. If people fail to meet work requirements, they could not only lose their health benefits through Medicaid, but they could also be barred from receiving subsidized coverage.
As Oklahoma plans its implementation of H.R.1’s work and community engagement requirements, it is critical that the state prioritize early and recurring outreach, automated data-driven verification supplemented by human checks, and broad, flexible exemptions to ensure that those who need an exemption can obtain one.
