
Progress since House Bill 4106, Oklahoma's law on mental health protocols for schools
Amid record levels of student suicidality and crisis, Oklahoma lawmakers partnered with Healthy Minds to pass House Bill 4106 in 2022 as one of the nation’s strongest laws for addressing student mental health crises.
Across Oklahoma, over 80% of middle and high schoolers reported moderate or high depressive symptoms, and one in ten had made a suicide plan in the past year, according to recent survey data.
Schools can be a critical lifeline for students who are suicidal or in crisis. When schools are prepared, they can help connect young people with ongoing support in the community.
Research has proven how students’ mental health and academic success are connected: one study showed a link between reading difficulties and anxiety and depression. And another found improvement in school climate and a reduction in disciplinary incidents as a result of school-based mental health programs.
Recognizing schools' integral role in youth mental health, HB 4106 required every school district to partner with a local mental health organization to develop a protocol for responding to students in suicidal and mental health crisis.
While school districts’ progress so far has been uneven across the state, early evidence suggests the legislation has prompted meaningful improvements in how schools and communities are equipped to respond to students’ mental health challenges.
To assess the impact of HB 4106 since it became law, we interviewed school districts and community mental health organizations across both rural and urban areas of the state. In this report, we outline recommendations to build on the progress school districts and community mental health organizations have made and address barriers that have prevented more widespread compliance with the law.
Key takeaways
- Most school districts — 80% — have submitted mental health crisis protocols in accordance with HB 4106. But many still need to be revised to satisfy requirements of the law: of the protocols reviewed by the state agencies charged with overseeing implementation, only 40% met all requirements.
- Community mental health organizations said HB 4106 has resulted in new or strengthened partnerships with schools, including increased referrals from schools. One Certified Community Behavioral Health Clinic (CCBHC) reported a 490% increase in referrals received from schools since the passage of HB 4106.
- Oklahoma would benefit from additional funding and staff to expand state agencies’ capacity to offer rigorous training and technical assistance that helps Oklahoma districts craft and implement crisis response protocols.
Requirements for districts under HB 4106
HB 4106, by Rep. Mark Vancuren (R-Owasso) and Sen. Dewayne Pemberton (R-Muskogee), required every school district to develop and submit a comprehensive crisis response protocol in partnership with local Certified Community Behavioral Health Clinics (CCBHCs).
To be considered in compliance with HB 4106, school districts must work with their local CCBHC or at least one local mental health organization certified by the Oklahoma Department of Mental Health and Substance Abuse Services (ODMHSAS), and must develop a crisis protocol that includes the following requirement:
- A definition of a mental health crisis, involving stipulations around potential for harm to self or others
- A process for how school staff can identify a mental health crisis
- An outline of non-punitive steps to safeguard student health and safety in response to a mental health crisis
- A list of local treatment providers and resources to support students and families in mental health crisis and ensure appropriate treatment referrals
- A process for notifying and involving parents or guardians during an actual or potential mental health crisis
- A process for how student privacy will be protected in compliance with state and federal laws
HB 4106 also requires school districts to use data from the OPNA, Oklahoma Prevention Needs Assessment (OPNA) survey to determine student needs and provide guidance on prevention programs. The OPNA surveys students in grades, 6, 8, 10, 12 and is given with parent permission to measure students’ risk factors around substance use, mental health needs, academic progress, and violence.
Ideally, districts and CCBHCs work together to review local OPNA results and use it to identify students’ mental health needs. From there, districts and CCBHCs should develop and adopt a suicide prevention plan that includes mental health screenings and targeted interventions when appropriate. Together, they should also develop and adopt crisis protocols, formalize their agreement with a memorandum of understanding, and educate CCBHC and district staff about carrying out the plans and protocols.
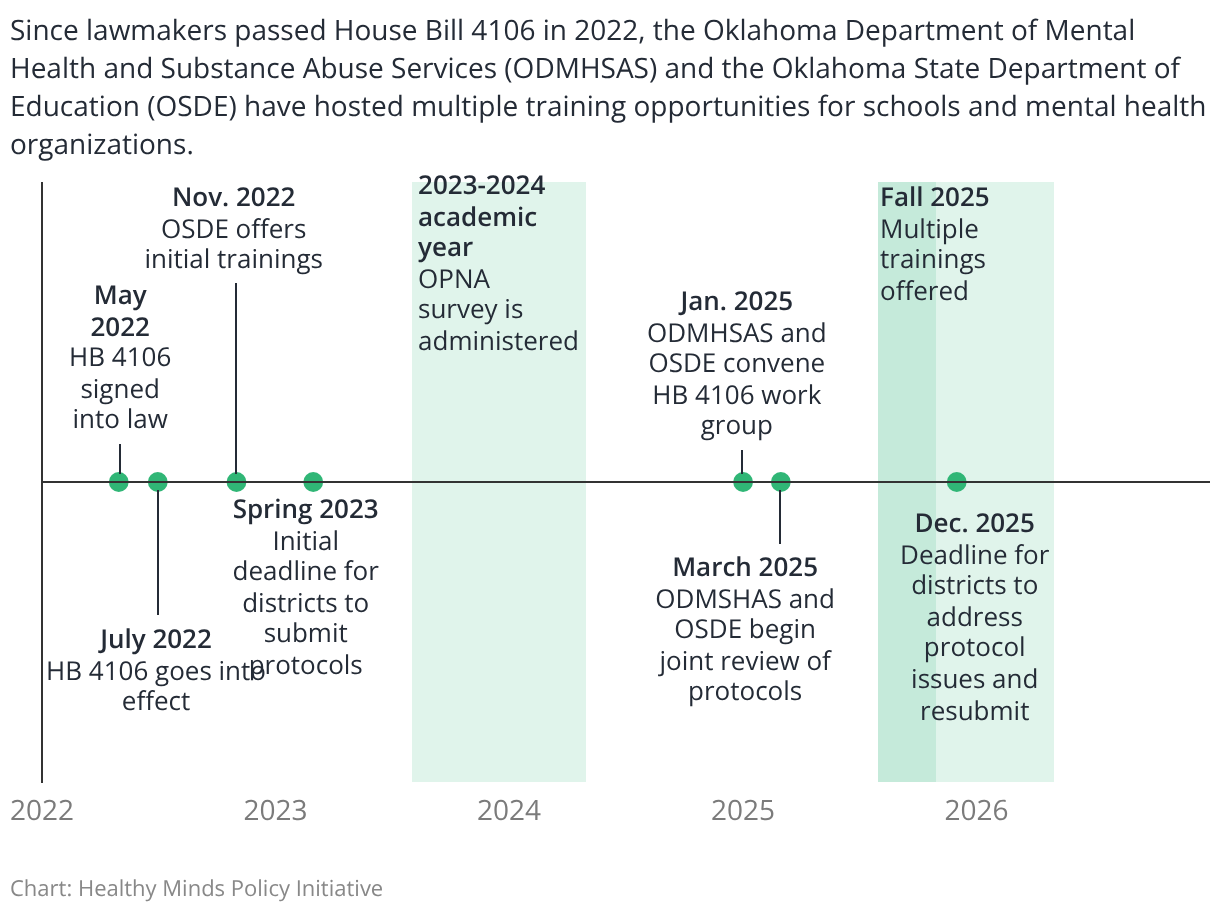
To support districts’ development of protocols that satisfy the law’s requirements, the Oklahoma State Department of Education and Oklahoma Department of Mental Health and Substance Abuse Services have offered multiple training opportunities for districts and mental health organizations. In addition to providing almost two dozen training opportunities, OSDE has created a mental health crisis response protocol template, which many districts used to develop their protocols.
House Bill 4106 implementation timeline
Assessing the law's impact
In our analysis, we sought to understand how many school districts had completed developing crisis response protocols, how well those protocols complied with the requirements of HB 4106, and what improvements districts and community mental health organizations have seen through their partnerships.
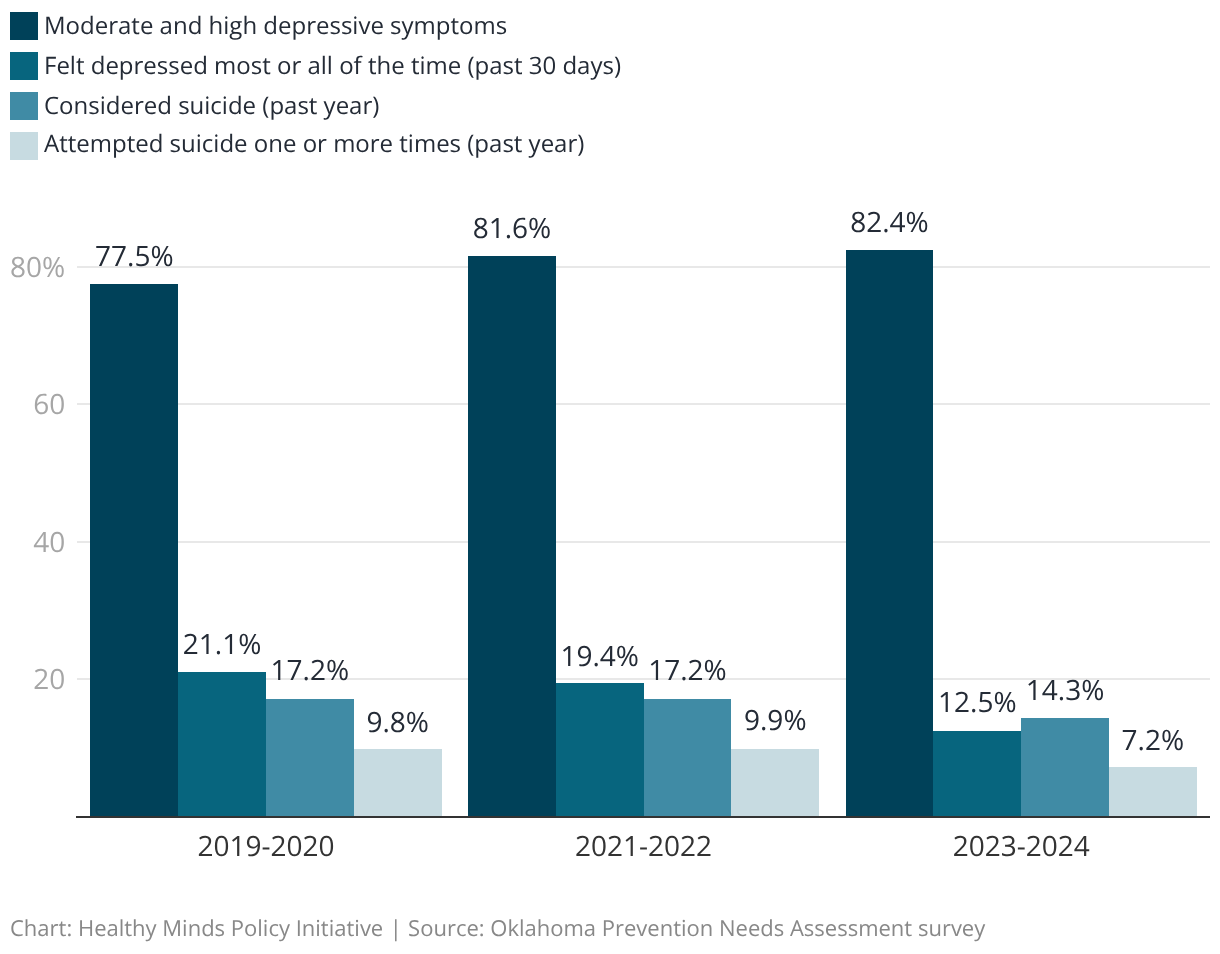
In the years since HB 4106 was passed, students’ rates of depressive symptoms have remained high. But Oklahoma has seen some modest declines in rates of suicide attempts among middle and high schoolers.
Depression and suicidality measures among Oklahoma middle and high school students
We also examined whether emergency room visits for youth in mental health crisis dropped since the law passed — one long-term outcome we would expect to see.
While we have not observed a decrease so far, it’s likely that we lack sufficient data to observe changes, especially since districts’ timelines for implementation vary widely.
Rates of protocol implementation and compliance
Overall, school districts are still developing their protocols, but compliance is uneven across the state.
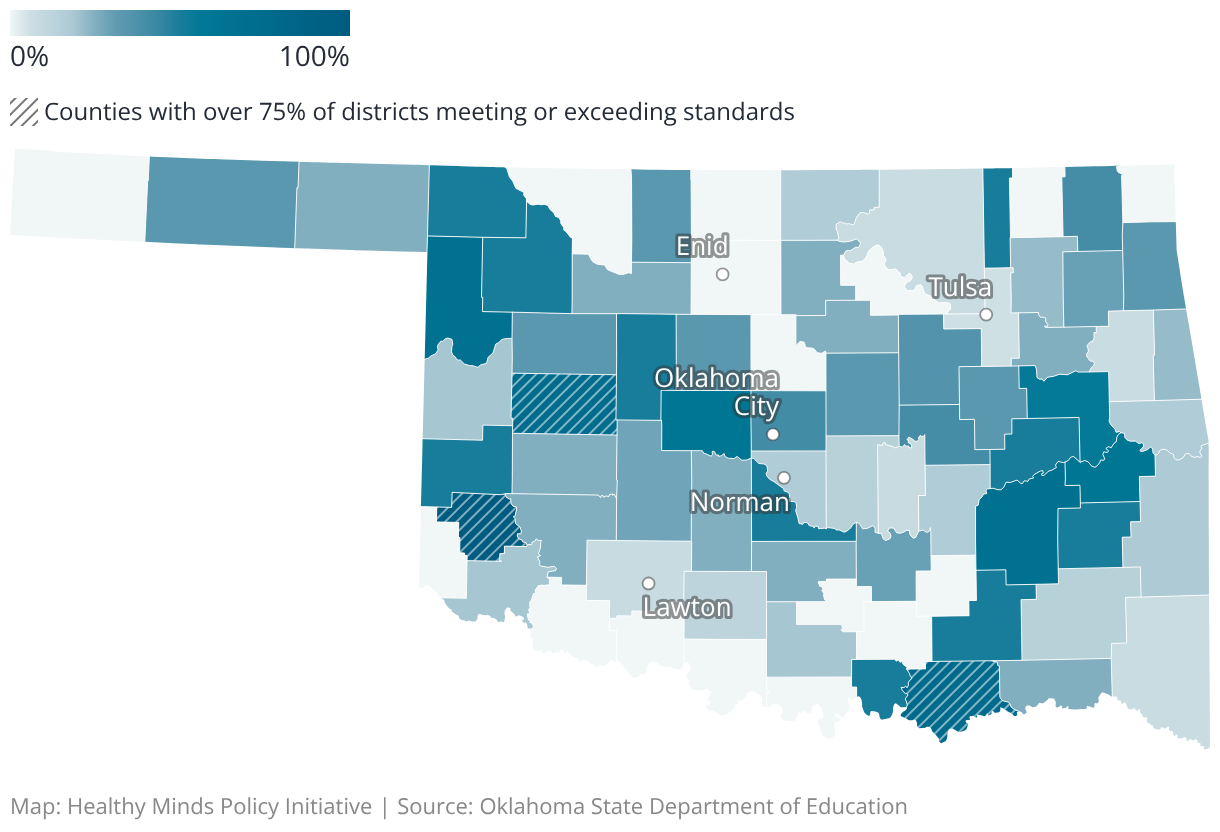
Three counties — Greer (100%), Bryan (78%), and Custer (75%) — have 75% or more of their districts demonstrating compliance with HB 4106.
Statewide, 21% of counties either have no districts that demonstrate compliance with HB 4106 or their protocols are currently under review by OSDE and ODMHSAS.
Percent of school districts that meet or exceed standards for HB 4106 protocols, by county
As of November 2025, 435 out of 543 districts (80%) had submitted protocols, of which 363 (85%) had been reviewed. Of the protocols reviewed, 145 (40%) were deemed to comply with HB 4106 requirements and the remaining 218 (60%) were found to have one or more compliance issues, requiring follow-up and verification by the OSDE.
In a survey conducted by OSDE, about 90% of school district respondents reported their districts have either partially or fully implemented their protocols.
Improved coordination with local behavioral health organizations
While implementation across the state is not yet complete, HB 4106’s required collaboration between school districts and a certified mental health organization has resulted in clear protocols and procedures allowing schools to effectively respond to students in crisis.
Some districts describe their new agreements with collaborating local mental health organizations as a critical “safety net,” ensuring they can confidently respond to a student mental health crisis. Several reported they are responding to student crises more effectively, engaging students in the appropriate crisis services, developing safety plans, and connecting families to follow-up services. Other school districts have used the HB 4106 requirements as an opportunity to strengthen existing relationships with their local community mental health organizations.
As a result of developing effective mental health crisis protocols, one community mental health organization has seen a 463% increase from 2022 to 2024 in crisis response calls from schools in their service area and an increase of 386% from 2021 to 2024 in all referrals for services from schools.
Another CCBHC reported an upward trend of referrals since they began working with schools to comply with the bill. From 2021 to 2025, their referrals from schools in the month of September increased by 490%. The bulk of that increase may be attributed to a greater number of schools with collaboration between their local CCBHCs stemming from HB 4106.
For example, the partnership between Shawnee Public Schools and its local CCBHC, CREOKS, illustrates the vision and intended impact of HB 4106.
Prior to HB 4106, Shawnee Public Schools did not have a formal partnership with CREOKS. Although they sometimes referred students and their families to CREOKS, it was not until HB 4106 was passed that they expanded their relationship with the provider to develop a formal mental health crisis response protocol.
According to a district representative, students in crisis were not receiving an immediate response due to a lack of uniform or effective crisis response processes. The passage of HB 4106 spurred Shawnee Public Schools to develop and formalize their crisis response protocol in collaboration with CREOKS. Today, school counselors know they have a direct line to CREOKS’ staff for crisis stabilization and assessment, either in-person or via telemedicine.
The CREOKS clinic in Shawnee received 211 referrals from Shawnee Public Schools during the 2022-2023 school year, the first year of HB 4106 implementation, and 471 referrals during the 2024-2025 school year, an increase of 123%. CREOKS provided 68 in-person crisis responses during the 2024-2025 school year when they officially became the Behavioral Intervention Services and Supports provider for Shawnee Public Schools, providing early identification of behavioral health issues, assessment and referral for treatment, and embedding behavioral health aides in school sites.
“A student experienced a significant mental health crisis at the end of the 24–25 school year. Thanks to the district’s established protocol, the school was able to respond quickly. Using the iPad provided by the CCBHC, the student was assessed at the school, allowing her mother to join the process in a safe and familiar environment. Both the student and her mother expressed how supported they felt and how much they appreciated avoiding an emergency room setting. … The impact of these efforts has been remarkable. When reviewing her most recent academic assessment scores compared to the previous year, we saw measurable academic improvement. Just as importantly, she now enjoys coming to school, has not engaged in behavioral outbursts, has not run from the building, and has maintained strong attendance. She is making friends and thriving in ways that once seemed unlikely.”
— CCHBC representative
Gaps and barriers
Many districts still have not yet developed a crisis response protocol that fully complies with the law. In our analysis, school officials and mental health providers pointed to several gaps and barriers that have prevented more widespread compliance.
Limited district and agency staff capacity
Current staffing is limited at both local and state level to support the implementation of HB 4106. Particularly in rural areas, school districts reported having insufficient staff time to fully attend to the requirements of HB 4106.
At the state level, the law required substantial roles for OSDE and ODMHSAS but did not provide for additional staffing, making it challenging for agencies to provide the amount of technical assistance needed to meet all the requirements. Despite this, the agencies provided many training and technical assistance opportunities for districts developing protocols.
There are no dedicated or funded positions to support the implementation of HB 4106 through ongoing training and technical assistance on mental health protocol development and application. Both state agencies have recognized a need for stronger state-level coordination and effort. ODMHSAS will be funding two contract positions (for this school year and next) through the Bipartisan Safer Communities Act to help OSDE review protocols, provide training and technical assistance to school and mental health organizations, and support overall HB 4106 implementation. However, these time-limited contract positions represent a short-term solution. There is a need for a more robust, sustainable long-term technical assistance and implementation support plans.
Limited capacity among mental health organizations and providers
Some CCBHCs serving large regions may have limited time to coordinate and collaborate with each school district in their region. CCBHCs serving regions that contain dozens of school districts may have difficulty in co-creating mental health crisis response protocols that are individually tailored and actionable for each school district.
CCBHCs in Oklahoma

Other challenges
Many school districts had difficulties submitting their protocols via the OSDE single sign-on portal, which resulted in delays to the review process. There is not a dedicated electronic platform for districts to submit their crisis protocols and the single sign-on platform used to collect protocols had several challenges including duplication of documents and issues with tracking submissions.
Some districts also reported confusion and delay caused by two different HB 4106-related policy guides issued by two different state-level organizations: OSDE, and the Oklahoma State School Boards Association (OSSBA). The OSSBA released a policy template for school board adoption that supported protocol implementation. However, state agency staff reported that school districts were confused about which template to use and submitted a school board policy template provided by the OSSBA rather than a district’s mental health crisis response protocol as required by the law.
Next steps for Oklahoma
Oklahoma can continue the progress districts and local community mental health organizations has started through HB 4106 and take steps to bring more communities into full compliance with the law.
Ideal response to a student mental health crisis

With more targeted supports for coordination and capacity, Oklahoma can fully achieve the vision of HB 4106. To this end, we recommend:
Expanded technical assistance and guidance
ODMHSAS and OSDE expand their implementation taskforce to include representatives from certified mental health organizations and school districts (urban, suburban, and rural) and charge them with developing two to three detailed protocol models based on best practices for responding to student crises in rural and urban settings.
The agencies should develop an evaluation plan to assess implementation outcomes, including the number of school-community partner crisis responses, student safety data, and other indicators such as emergency room utilization, school attendance, expulsions, and school performance.
We also recommend the agencies establish a robust, long-term technical assistance and training plan that offers support to schools and certified mental health organizations that includes the requirements of HB 4106, practice improvements, and monitoring progress. This may include coordination with OSSBA on communication with school districts about mental health protocols vs. board policies.
Improved compliance monitoring
OSDE should expand monitoring compliance of HB 4106 requirements for school districts to include districts’ work to train school administrators, teachers, support employees and school-based mental health providers on the school district’s protocols.
The agency should also ensure school district and mental health provider partners jointly review the protocol and working agreements every two years, using local OPNA survey results or similar.
Support for expanded staff capacity
Policymakers should increase funding for school districts to support expansion of staff capacity related to requirements of HB 4106. With more staffing devoted to developing and implementing strong crisis response protocols and building out other tiers of the mental health service continuum in schools, Oklahoma will see growth in services such as cost-effective preventative interventions.
Funding could be phased in over time and distributed via a competitive application process focused on developing resources in rural areas. If a rigorous evaluation demonstrates effectiveness, the grant program could be expanded to new areas of the state identified as high need.
Recognizing the challenges students face today, these recommendations will help Oklahoma schools and communities become better equipped to help students in crisis through the meaningful partnerships HB 4106 set out to foster.
